

Deep learning aided preoperative diagnosis of primary central nervous system lymphoma
- PMID: 38352223
- PMCID: PMC10863328
- DOI: 10.1016/j.isci.2024.109023
Deep learning aided preoperative diagnosis of primary central nervous system lymphoma
Abstract
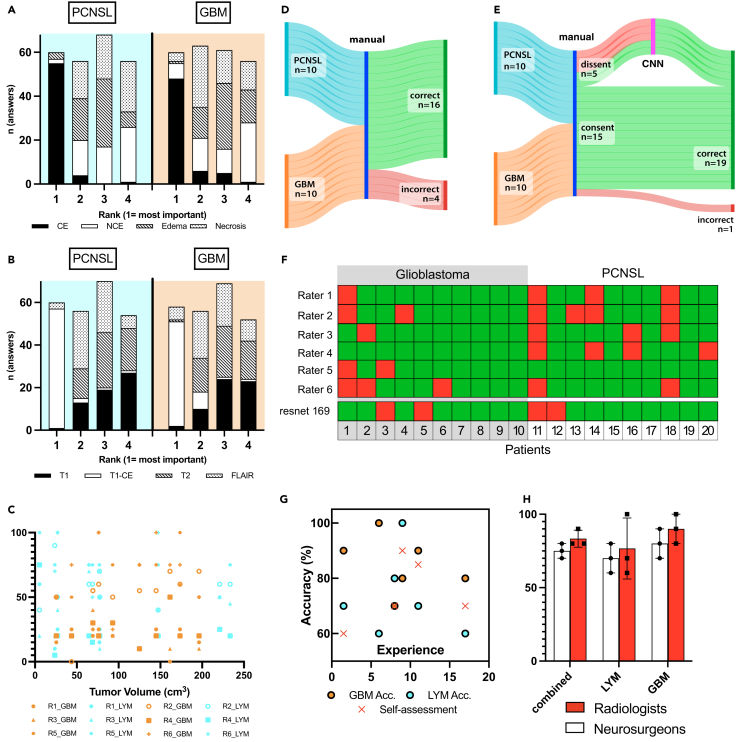
The preoperative distinction between glioblastoma (GBM) and primary central nervous system lymphoma (PCNSL) can be difficult, even for experts, but is highly relevant. We aimed to develop an easy-to-use algorithm, based on a convolutional neural network (CNN) to preoperatively discern PCNSL from GBM and systematically compare its performance to experienced neurosurgeons and radiologists. To this end, a CNN-based on DenseNet169 was trained with the magnetic resonance (MR)-imaging data of 68 PCNSL and 69 GBM patients and its performance compared to six trained experts on an external test set of 10 PCNSL and 10 GBM. Our neural network predicted PCNSL with an accuracy of 80% and a negative predictive value (NPV) of 0.8, exceeding the accuracy achieved by clinicians (73%, NPV 0.77). Combining expert rating with automated diagnosis in those cases where experts dissented yielded an accuracy of 95%. Our approach has the potential to significantly augment the preoperative radiological diagnosis of PCNSL.
Keywords: Diagnostic technique in health technology; Health sciences; Health technology; Internal medicine; Medical specialty; Medicine; Oncology; Radiology.
© 2024 The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
Associated data
LinkOut - more resources
Full Text Sources
