

The Age-Male-Albumin-Bilirubin-Platelets (aMAP) Risk Score Predicts Liver Metastasis Following Surgery for Breast Cancer in Chinese Population: A Retrospective Study
- PMID: 38352235
- PMCID: PMC10861995
- DOI: 10.2147/ITT.S446545
The Age-Male-Albumin-Bilirubin-Platelets (aMAP) Risk Score Predicts Liver Metastasis Following Surgery for Breast Cancer in Chinese Population: A Retrospective Study
Abstract
Objective: The current study is conducted to investigate the potential prognostic value of the age-male-albumin-bilirubin-platelets (aMAP) score in breast cancer patients with liver metastasis after surgery.
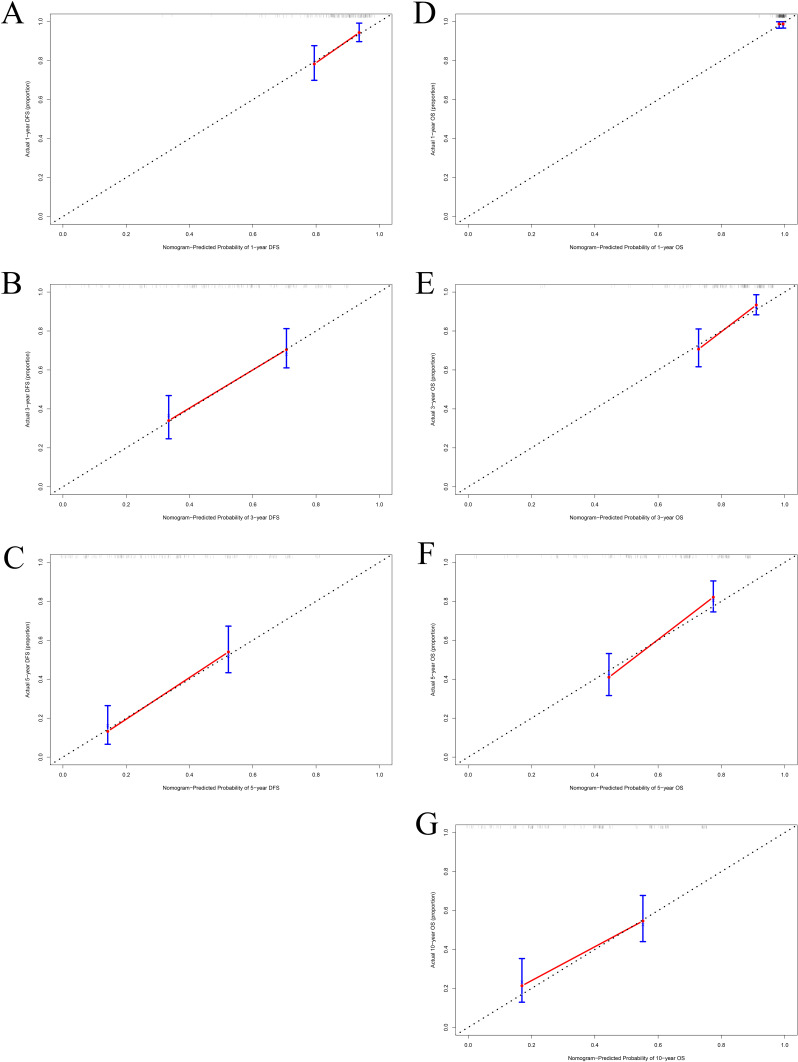
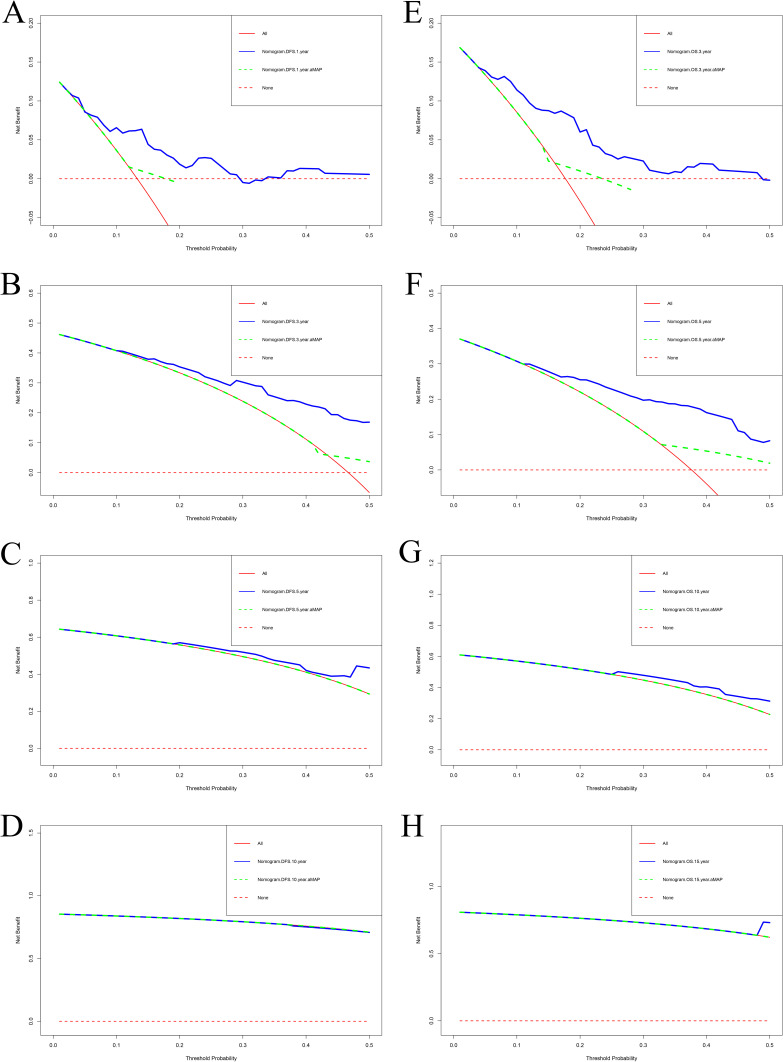
Methods: This is a retrospective study of 178 breast cancer patients who developed liver metastasis after surgery. These patients were treated and followed up from 2000 to 2018 at our hospital. The aMAP risk score was estimated in accordance with the following formula: . The optimal cutoff value of the aMAP was evaluated via X-tile. Kaplan-Meier, Log-rank and Cox proportional hazards regression models were applied to determine the clinical influence of the aMAP score on the survival outcomes. The nomogram models were established by multivariate analyses. The calibration curves and decision curve analysis were applied to evaluate the estimated performance of the nomogram models.
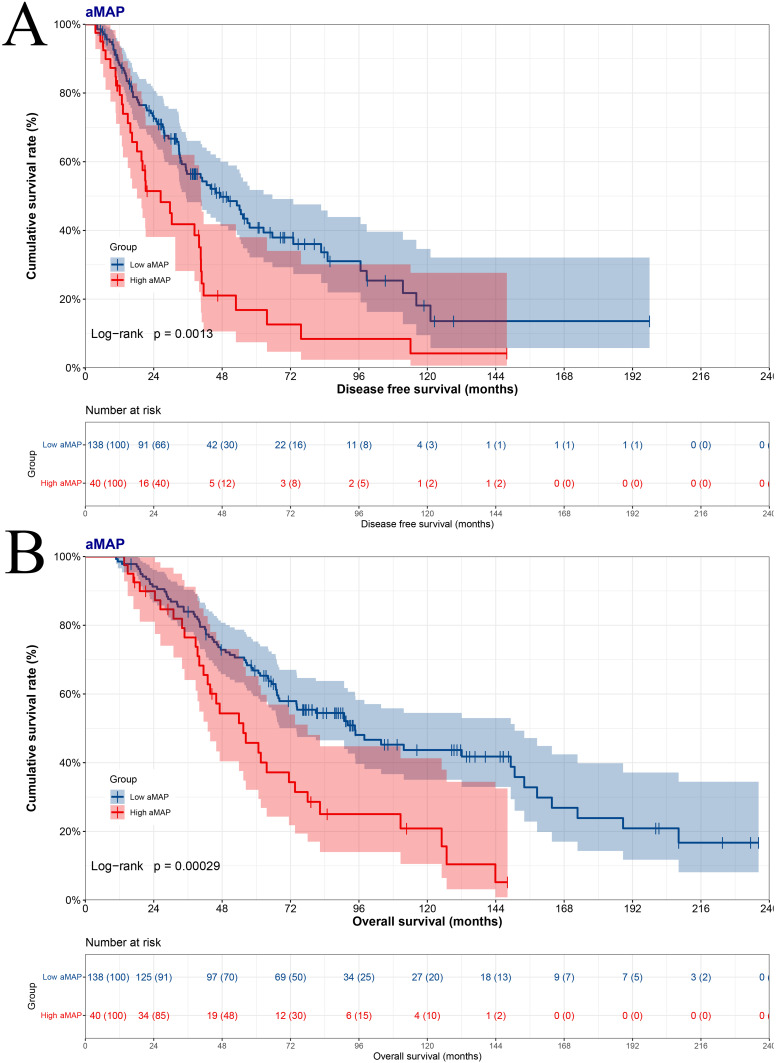
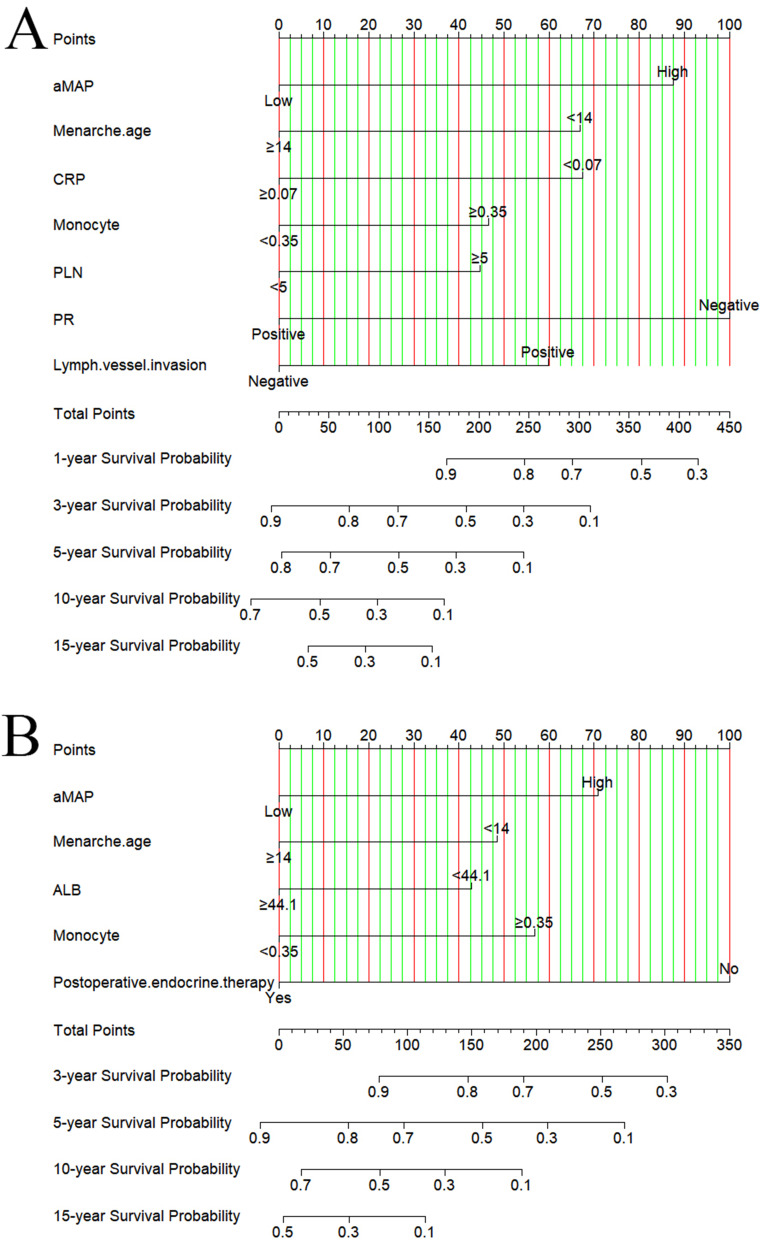
Results: A total of 178 breast cancer patients were divided into low aMAP score group (<47.6) and high aMAP score group (≥47.6) via X-tile plots. The aMAP score was a potential prognostic factor in multivariate analysis. The median disease free survival (p=0.0013) and overall survival (p=0.0003) in low aMAP score group were longer than in high aMAP score group. The nomograms were constructed to predict the DFS with a C-index of 0.722 (95% CI, 0.673-0.771), and the OS with a C-index of 0.708 (95% CI, 0.661-0.755). The aMAP-based nomograms had good predictive performance.
Conclusion: The aMAP score is a potential prognostic factor in breast cancer with liver metastasis after surgery. The aMAP score-based nomograms were conducive to discriminate patients at high risks of liver metastasis and develop adjuvant treatment and prevention strategies.
Keywords: aMAP score; albumin; breast cancer; liver metastasis; prognosis.
© 2024 Chen et al.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Giuliano M, Schettini F, Rognoni C, et al. Endocrine treatment versus chemotherapy in postmenopausal women with hormone receptor-positive, HER2-negative, metastatic breast cancer: a systematic review and network meta-analysis. Lancet Oncol. 2019;20(10):1360–1369. doi: 10.1016/S1470-2045(19)30420-6 - DOI - PubMed
LinkOut - more resources
Full Text Sources
