

Projecting the 10-year costs of care and mortality burden of depression until 2032: a Markov modelling study developed from real-world data
- PMID: 38352243
- PMCID: PMC10862399
- DOI: 10.1016/j.lanwpc.2024.101026
Projecting the 10-year costs of care and mortality burden of depression until 2032: a Markov modelling study developed from real-world data
Abstract
Background: Based on real-world data, we developed a 10-year prediction model to estimate the burden among patients with depression from the public healthcare system payer's perspective to inform early resource planning in Hong Kong.
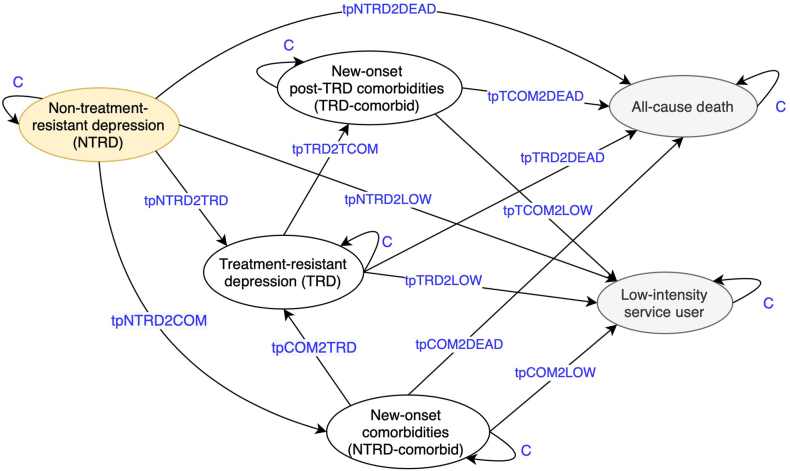
Methods: We developed a Markov cohort model with yearly cycles specifically capturing the pathway of treatment-resistant depression (TRD) and comorbidity development along the disease course. Projected from 2023 to 2032, primary outcomes included costs of all-cause and psychiatric care, and secondary outcomes were all-cause deaths, years of life lived, and quality-adjusted life-years. Using the territory-wide electronic medical records, we identified 25,190 patients aged ≥10 years with newly diagnosed depression from 2014 to 2016 with follow-up until 2020 to observe the real-world time-to-event pattern, based on which costs and time-varying transition inputs were derived using negative binomial modelling and parametric survival analysis. We applied the model as both closed cohort, which studied a fixed cohort of incident patients in 2023, and open cohort, which introduced incident patients by year from 2014 to 2032. Utilities and annual new patients were from published sources.
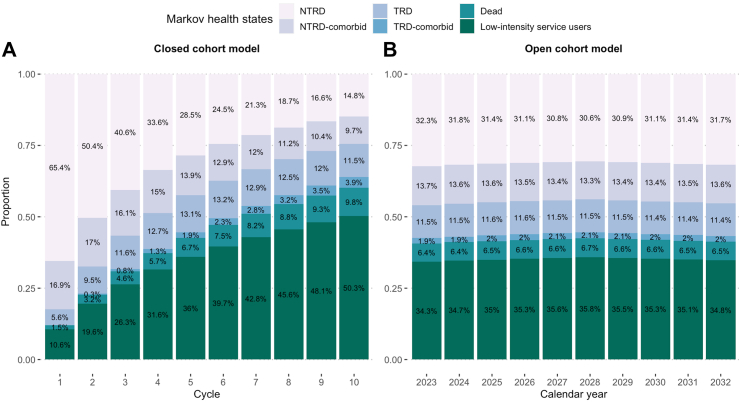
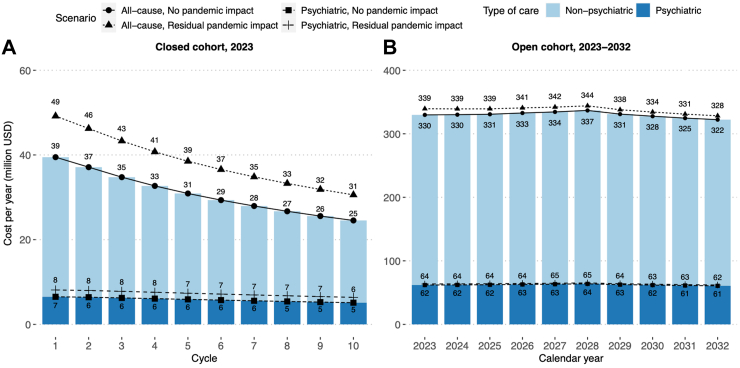
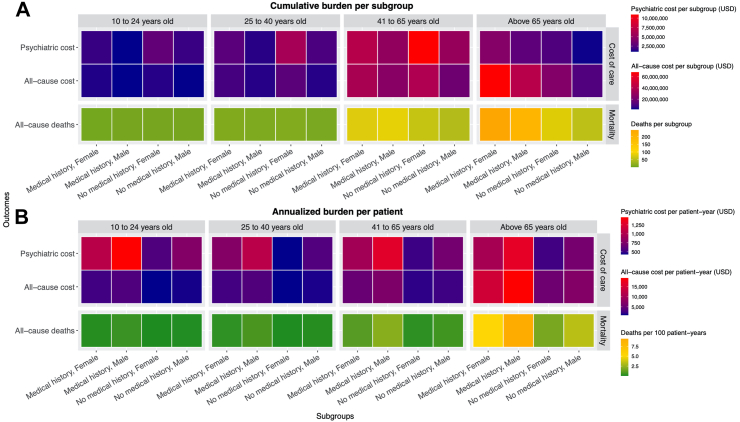
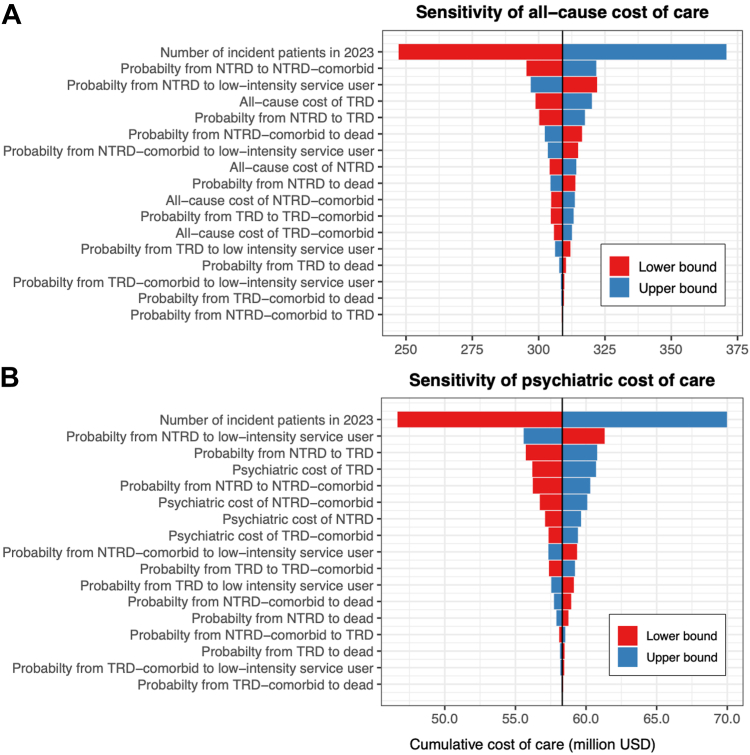
Findings: With 9217 new patients in 2023, our closed cohort model projected the 10-year cumulative costs of all-cause and psychiatric care to reach US$309.0 million and US$58.3 million, respectively, with 899 deaths (case fatality rate: 9.8%) by 2032. In our open cohort model, 55,849-57,896 active prevalent cases would cost more than US$322.3 million and US$60.7 million, respectively, with more than 943 deaths annually from 2023 to 2032. Fewer than 20% of cases would live with TRD or comorbidities but contribute 31-54% of the costs. The greatest collective burden would occur in women aged above 40, but men aged above 65 and below 25 with medical history would have the highest costs per patient-year. The key cost drivers were relevant to the early disease stages.
Interpretation: A limited proportion of patients would develop TRD and comorbidities but contribute to a high proportion of costs, which necessitates appropriate attention and resource allocation. Our projection also demonstrates the application of real-world data to model long-term costs and mortality, which aid policymakers anticipate foreseeable burden and undertake budget planning to prepare for the care need in alternative scenarios.
Funding: Research Impact Fund from the University Grants Committee, Research Grants Council with matching fund from the Hong Kong Association of Pharmaceutical Industry (R7007-22).
Keywords: Burden projection; Comorbidities; Cost; Depression; Health policy; Mortality; Real-world data; Real-world evidence; Time-varying Markov model; Treatment-resistant depression.
© 2024 The Authors.
Conflict of interest statement
X Li received research grants from Hong Kong Health and Medical Research Fund (HMRF, HMRF Fellowship Scheme, HKSAR), Research Grants Council Early Career Scheme (RGC/ECS, HKSAR), Janssen and Pfizer; internal funding from the University of Hong Kong; consultancy fees from Merck Sharp & Dohme and Pfizer; she is also a non-executive director of Advanced Data Analytics for Medical Science (ADAMS) Limited Hong Kong, all are unrelated to this work; H Luo received research grants Research Grants Council Early Career Scheme (RGC/ECS, HKSAR) unrelated to this work. EWY Chan reports grants from Research Grants Council, Research Fund Secretariat of the Food and Health Bureau, National Natural Science Fund of China, Wellcome Trust, Bayer, Amgen, Bristol-Myers Squibb, Janssen, Takeda, Narcotics Division of the Security Bureau of Hong Kong, honorarium from Hospital Authority, outside the submitted work; ICK Wong received research funding outside the submitted work from Amgen, Bristol-Myers Squibb, Pfizer, Janssen, Bayer, GSK, Novartis, Takeda, the Hong Kong RGC, and the Hong Kong Health and Medical Research Fund, National Institute for Health Research in England, European Commission, National Health and Medical Research Council in Australia, The European Union's Seventh Framework Programme for research technological development, and has also received consulting fees from IQVIA, the WHO and expert testimony for Appeal Court in Hong Kong over the past three years. He is also a non-executive director of Jacobson Medical Hong Kong, and founder and director of Therakind Limited (United Kingdom), Advanced Data Analytics for Medical Science (ADAMS) Limited (Hong Kong), Asia Medicine Regulatory Affairs (AMERA) Services Limited and OCUS Innovation Limited (Hong Kong, Ireland and United Kingdom).
Figures
References
-
- World Health Organization . 2011. Global burden of mental disorders and the need for a comprehensive, coordinated response from health and social sectors at the country level–Report by the Secretariat. Geneva.
LinkOut - more resources
Full Text Sources
