

This is a preprint.
Pediatric human nose organoids demonstrate greater susceptibility, epithelial responses, and cytotoxicity than adults during RSV infection
- PMID: 38352333
- PMCID: PMC10862794
- DOI: 10.1101/2024.02.01.578466
Pediatric human nose organoids demonstrate greater susceptibility, epithelial responses, and cytotoxicity than adults during RSV infection
Update in
-
Infant-derived human nasal organoids exhibit relatively increased susceptibility, epithelial responses, and cytotoxicity during RSV infection.J Infect. 2024 Dec;89(6):106305. doi: 10.1016/j.jinf.2024.106305. Epub 2024 Oct 9. J Infect. 2024. PMID: 39389204 Free PMC article.
Abstract
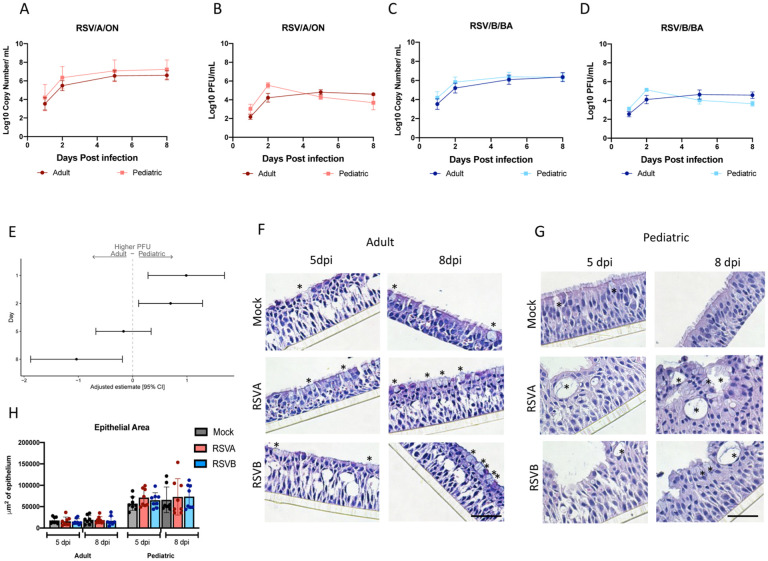
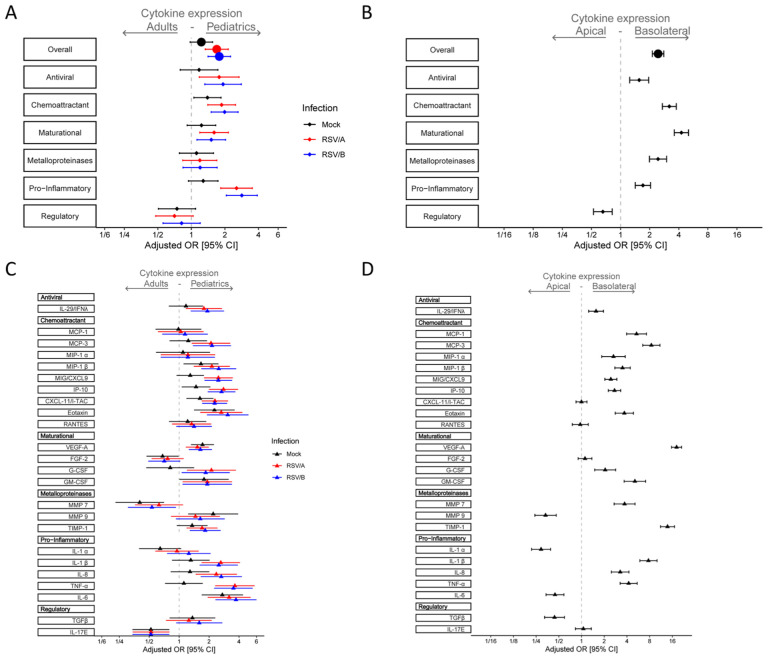
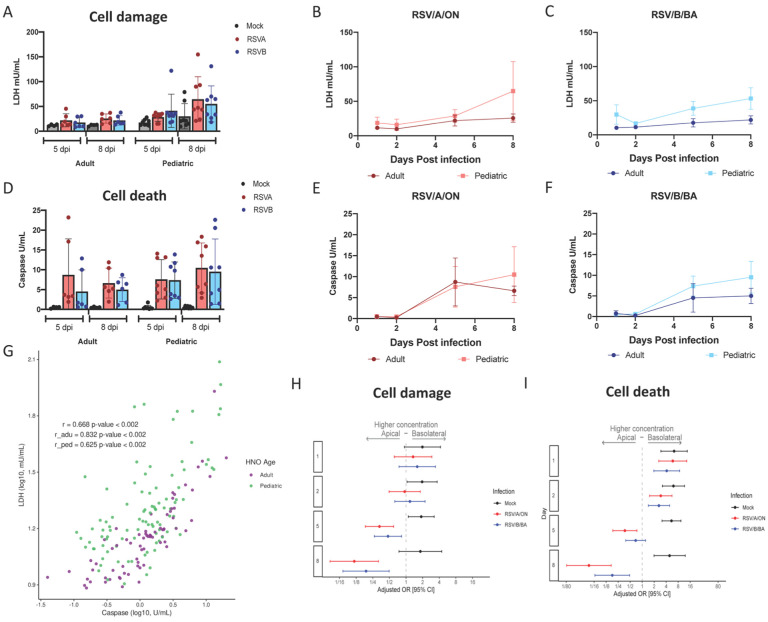
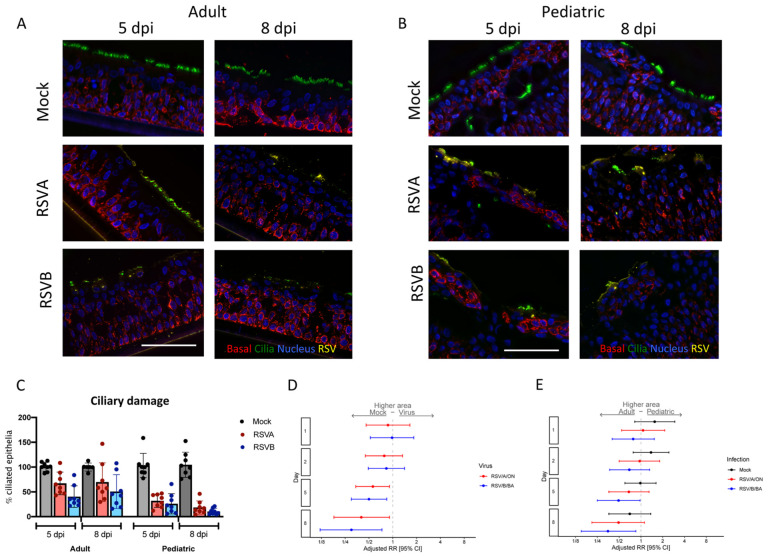
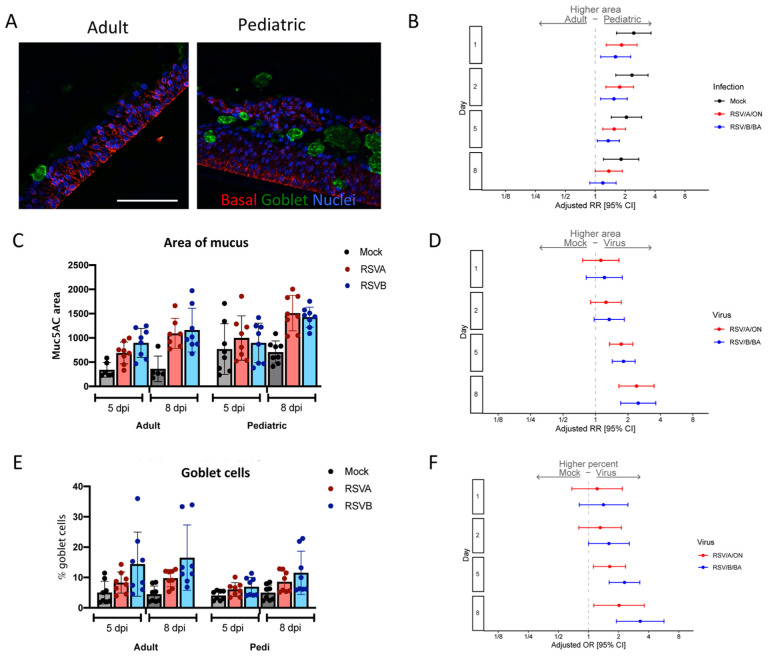
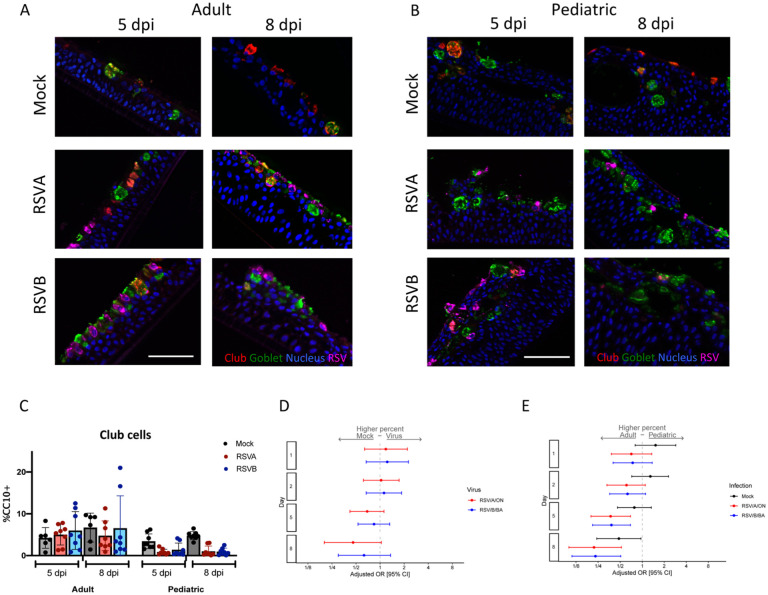
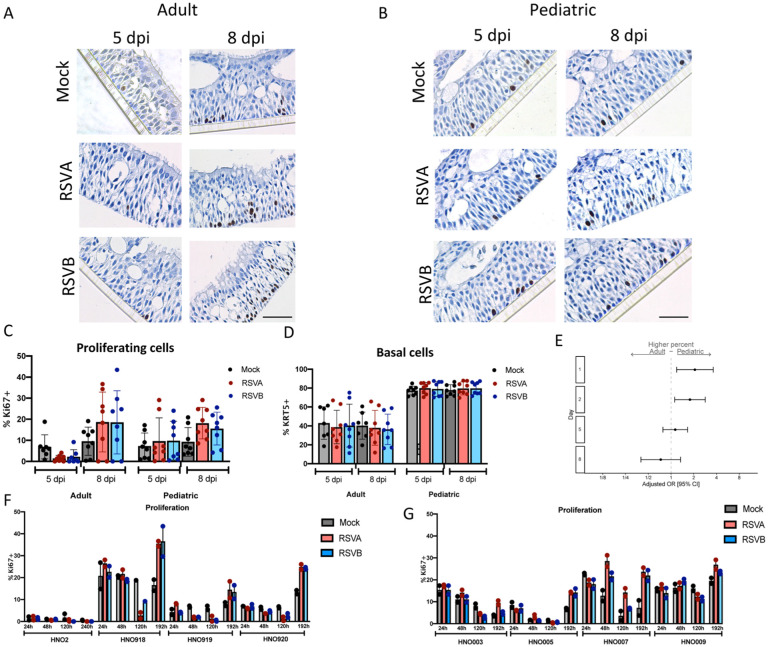
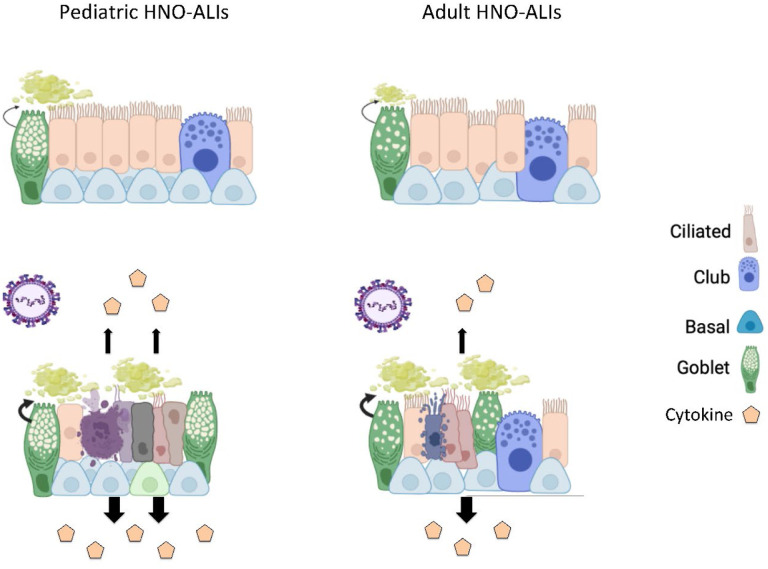
Respiratory syncytial virus (RSV) is a common cause of respiratory infections, causing significant morbidity and mortality, especially in young children. Why RSV infection in children is more severe as compared to healthy adults is not fully understood. In the present study, we infect both pediatric and adult human nose organoid-air liquid interface (HNO-ALIs) cell lines with two contemporary RSV isolates and demonstrate how they differ in virus replication, induction of the epithelial cytokine response, cell injury, and remodeling. Pediatric HNO-ALIs were more susceptible to early RSV replication, elicited a greater overall cytokine response, demonstrated enhanced mucous production, and manifested greater cellular damage compared to their adult counterparts. Adult HNO-ALIs displayed enhanced mucus production and robust cytokine response that was well controlled by superior regulatory cytokine response and possibly resulted in lower cellular damage than in pediatric lines. Taken together, our data suggest substantial differences in how pediatric and adult upper respiratory tract epithelium responds to RSV infection. These differences in epithelial cellular response can lead to poor mucociliary clearance and predispose infants to a worse respiratory outcome of RSV infection.
Conflict of interest statement
Conflict of interest: The authors declare no conflicts of interest.
Figures
References
-
- Meissner HC. Viral Bronchiolitis in Children. N Engl J Med. 2016;374(1):62–72. - PubMed
-
- Greenberg SB. Viral pneumonia. Infect Dis Clin North Am. 1991;5(3):603–21. - PubMed
-
- Smith DK, Seales S, Budzik C. Respiratory Syncytial Virus Bronchiolitis in Children. Am Fam Physician. 2017;95(2):94–99. - PubMed
-
- Glezen WP, et al. Risk of primary infection and reinfection with respiratory syncytial virus. Am J Dis Child. 1986;140(6):543–6. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources