

This is a preprint.
A vagal influence on schizophrenia? A nationwide retrospective cohort of vagotomized individuals
- PMID: 38352405
- PMCID: PMC10862985
- DOI: 10.1101/2024.01.30.24301418
A vagal influence on schizophrenia? A nationwide retrospective cohort of vagotomized individuals
Abstract
Background and objectives: Emerging preclinical evidence suggests that vagal signals contribute to the development of schizophrenia-related abnormalities in brain and behavior. Whether vagal communication in general, and its impairment in particular, is a risk factor for schizophrenia in humans remains, however, unclear. Vagotomy, the surgical lesion of the vagus nerve, was routinely performed as a treatment for peptic ulcer before modern treatment options were available. Hence, the primary aim of this study was to investigate whether vagotomy modulates the subsequent risk of developing schizophrenia. Moreover, given the existence of diverse vagotomy techniques (i.e., "truncal" or "selective"), our secondary goal was to test whether the extent of denervation modulates the risk of schizophrenia.
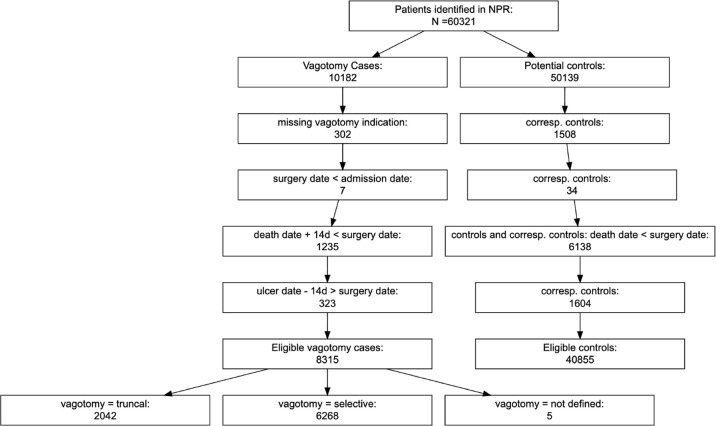
Methods: Using a nationwide retrospective matched cohort design, we identified 8,315 vagotomized individuals from the Swedish National Patient Register during the period 1970-2020 and 40,855 non-vagotomized individuals matching for age, sex and type of peptic ulcer. The risk of being diagnosed with schizophrenia and associated psychoses (ICD10 codes F20-29) was analyzed using Cox proportional hazards regression models, including death as competing risk.
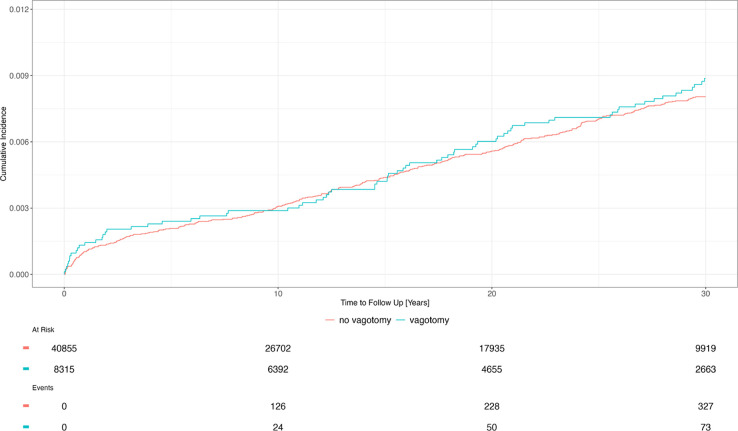
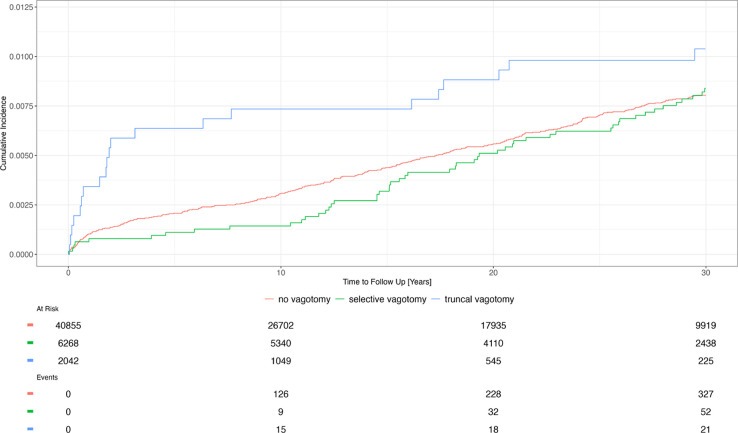
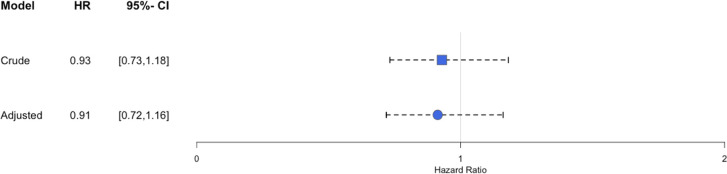
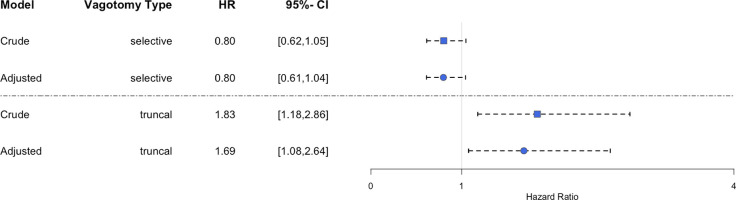
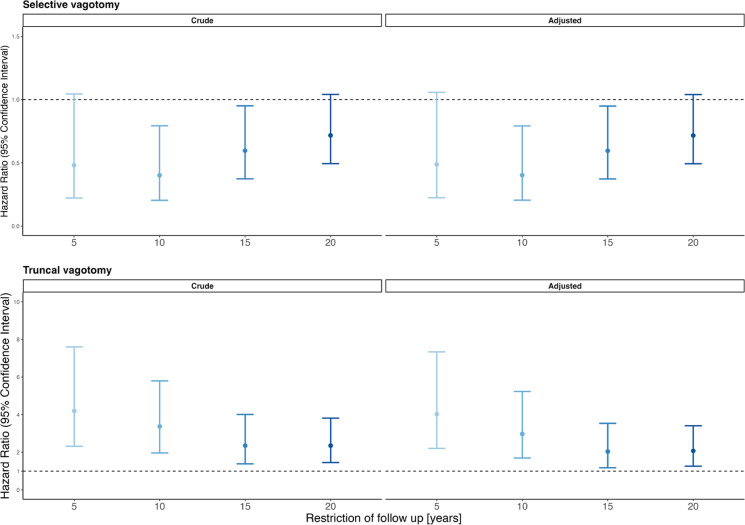
Results: When considering all types of vagotomy together, vagotomy was not significantly associated with schizophrenia (HR: 0.91 [0.72; 1.16]). However, truncal vagotomy (which denervates all subdiaphragmatic organs) significantly increased the risk of developing schizophrenia by 69% (HR: 1.69 [1.08; 2.64]), whereas selective vagotomy (which only denervates the stomach) showed no significant association (HR: 0.80 [0.61; 1.04]).
Discussion: Our results provide epidemiological support for the hypothesis that impairments in vagal functions could increase the risk of schizophrenia. Notably, the finding that truncal but not selective vagotomy is associated with an increased risk of schizophrenia raises the possibility that the activity of subdiaphragmatic non-gastric vagal branches may be of particular relevance for the development of schizophrenia.
Keywords: cohort study; gut-brain axis; schizophrenia; ulcer; vagus nerve.
Conflict of interest statement
5Conflicts of interests The authors have no conflicts to declare.
Figures
Similar articles
-
Vagotomy and Parkinson disease: A Swedish register-based matched-cohort study.Neurology. 2017 May 23;88(21):1996-2002. doi: 10.1212/WNL.0000000000003961. Epub 2017 Apr 26. Neurology. 2017. PMID: 28446653 Free PMC article.
-
Association of Vagotomy and Decreased Risk of Subsequent Ischemic Stroke in Complicated Peptic Ulcer Patients: an Asian Population Study.World J Surg. 2017 Dec;41(12):3171-3179. doi: 10.1007/s00268-017-4127-z. World J Surg. 2017. PMID: 28726018
-
MALT Lymphoma, Stress Ulcer and Cholinergic Nerves from the Viewpoint of Bilateral and Unilateral Truncal Vagotomy and Substance P.Curr Pharm Des. 2018;24(18):1961-1965. doi: 10.2174/1381612824666180516103027. Curr Pharm Des. 2018. PMID: 29766790 Review.
-
A comparative study of subsequent liver cirrhosis risk in non-Helicobacter pylori-infected peptic ulcer patients with and without vagotomy: An Asian population cohort study.J Gastroenterol Hepatol. 2019 Feb;34(2):376-382. doi: 10.1111/jgh.14440. Epub 2018 Oct 3. J Gastroenterol Hepatol. 2019. PMID: 30101458
-
Cellular Energetical Actions of "Chemical" and "Surgical" Vagotomy in Gastrointestinal Mucosal Damage and Protection: Similarities, Differences and Significance for Brain-Gut Function.Curr Neuropharmacol. 2016;14(8):901-913. doi: 10.2174/1570159x14666160719121725. Curr Neuropharmacol. 2016. PMID: 27440445 Free PMC article. Review.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources