

A Lateral Fracture Line Affects Femoral Trochanteric Fracture Instability and Swing Motion of the Intramedullary Nail: A Biomechanical Study
- PMID: 38352644
- PMCID: PMC10860993
- DOI: 10.2106/JBJS.OA.23.00118
A Lateral Fracture Line Affects Femoral Trochanteric Fracture Instability and Swing Motion of the Intramedullary Nail: A Biomechanical Study
Abstract
Background: An unstable trochanteric femoral fracture is a serious injury, with a 1-year mortality rate of 5.4% to 24.9%, for which there is currently no standard treatment method. The lag screw insertion site is one of the primary contact areas between the cortical bone and an intramedullary nail. We hypothesized that a posterolateral fracture causes intramedullary nail instability when the posterolateral fracture line interferes with lag screw insertion. The purpose of the present study was to investigate the effect of posterolateral fracture line morphology on intramedullary nail stability by simulating unstable trochanteric femoral fractures with a posterolateral fracture fragment.
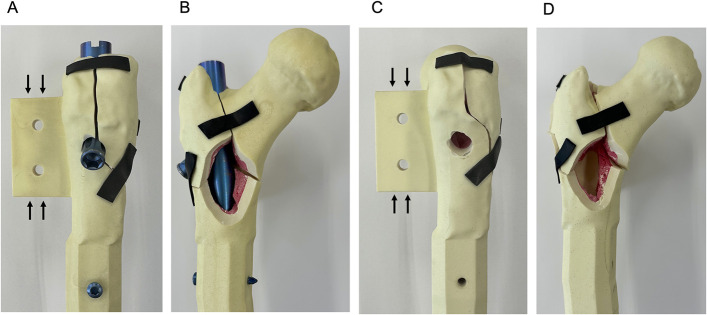
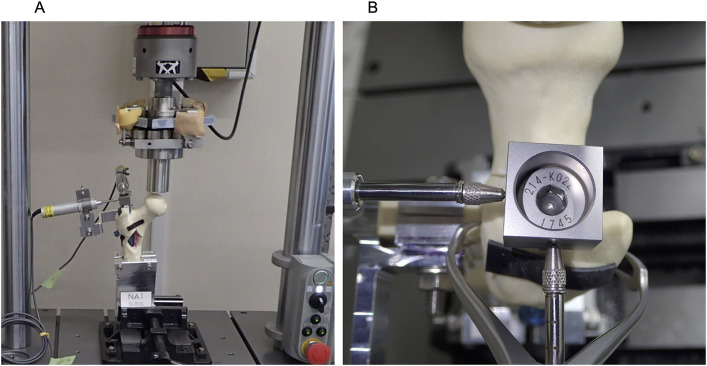
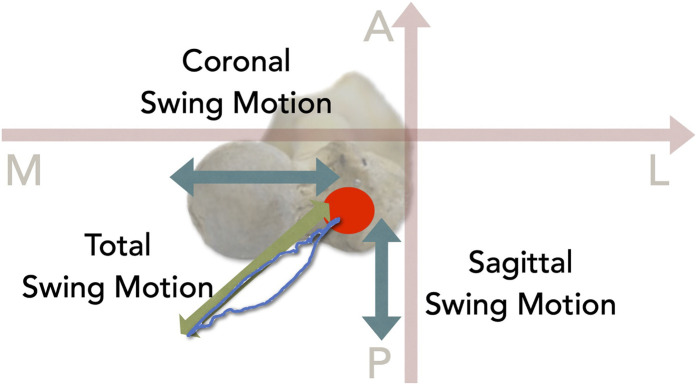
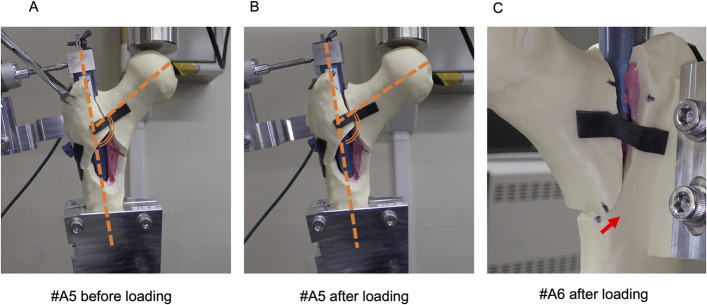
Methods: Eighteen custom-made synthetic osteoporotic bone samples were used in the present study. Nine samples had a posterolateral fracture line interfering with the lag screw insertion hole (Fracture A), and the other 9 had a fracture line 10 mm away from the hole (Fracture B). Cyclic loading (750 N) was applied to the femoral head 1,500 times. Movement of the end cap attached to the intramedullary nail was recorded. The amplitudes of motion in the coronal plane (coronal swing motion), sagittal plane (sagittal swing motion), and axial plane (total swing motion) were evaluated. The change in the neck-shaft angle was evaluated on photographs that were made before and after the test. Medial cortical displacement was measured before and after the test.
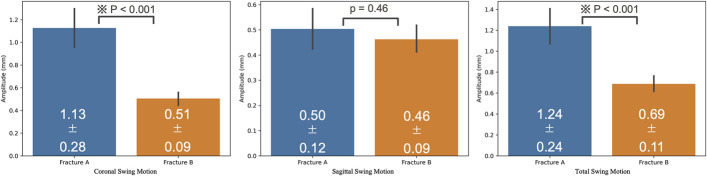
Results: Two Fracture-A samples were excluded because the amplitude of sagittal swing motion was too large. The mean values for coronal, sagittal, and total swing motion were 1.13 ± 0.28 mm and 0.51 ± 0.09 mm (p < 0.001), 0.50 ± 0.12 mm and 0.46 ± 0.09 mm (p = 0.46), and 1.24 ± 0.24 mm and 0.69 ± 0.11 mm (p < 0.001) for Fractures A and B, respectively. The mean neck-shaft angle change was -8.29° ± 2.69° and -3.56° ± 2.35° for Fractures A and B, respectively (p = 0.002). The mean displacement of the medial cortex was 0.38 ± 1.12 mm and 0.12 ± 0.37 mm for Fractures A and B, respectively (p = 0.57).
Conclusions: This study showed that an unstable trochanteric femoral fracture with a posterolateral fracture line that interferes with the lag screw insertion holes is a risk factor for increased intramedullary nail instability.
Copyright © 2024 The Authors. Published by The Journal of Bone and Joint Surgery, Incorporated. All rights reserved.
Conflict of interest statement
Disclosure: This study was funded by Teijin Nakashima Medical Co., Ltd. (the manufacturer of the intramedullary nails used in the study), and also partly supported by a Grant-in-Aid for Scientific Research (19K18471) from the Ministry of Education, Culture, Sports, Science, and Technology of Japan, and a Grant-in-Aid for Research (2213035) from Nagoya City University. The Article Processing Charge for open access publication was funded by Teijin Nakashima Medical Co., Ltd. The Disclosure of Potential Conflicts of Interest forms are provided with the online version of the article (http://links.lww.com/JBJSOA/A601).
Figures
References
-
- McLeod K, Brodie MP, Fahey PP, Gray RA. Long-term survival of surgically treated hip fracture in an Australian regional hospital. Anaesth Intensive Care. 2005. Dec;33(6):749-55. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous