

Accuracy of the 10 μg desmopressin test for differential diagnosis of Cushing syndrome: a systematic review and meta-analysis
- PMID: 38352712
- PMCID: PMC10861662
- DOI: 10.3389/fendo.2024.1332120
Accuracy of the 10 μg desmopressin test for differential diagnosis of Cushing syndrome: a systematic review and meta-analysis
Abstract
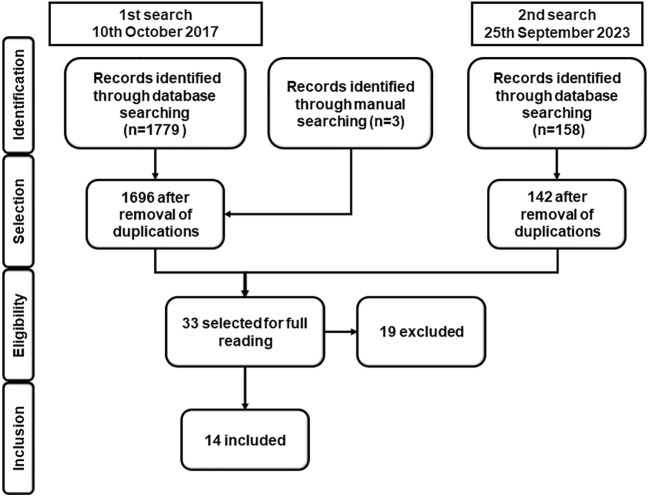
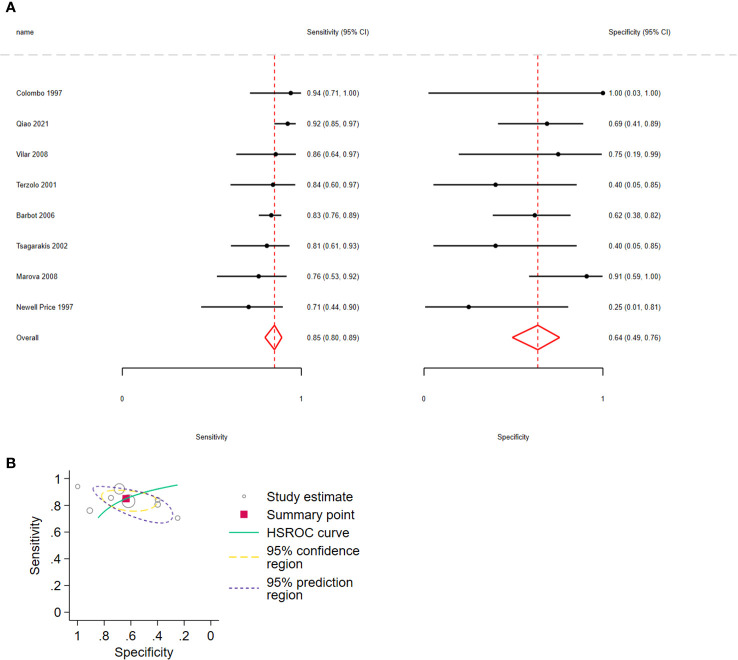
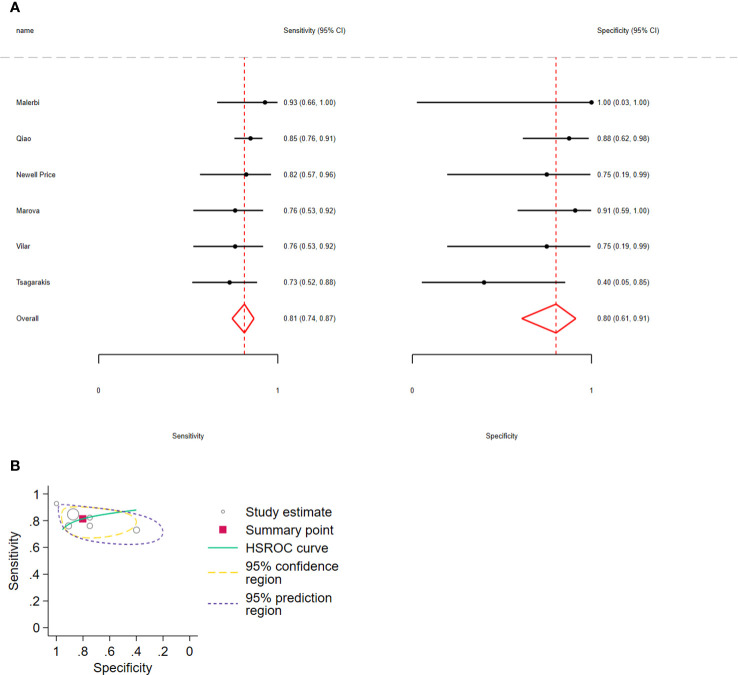
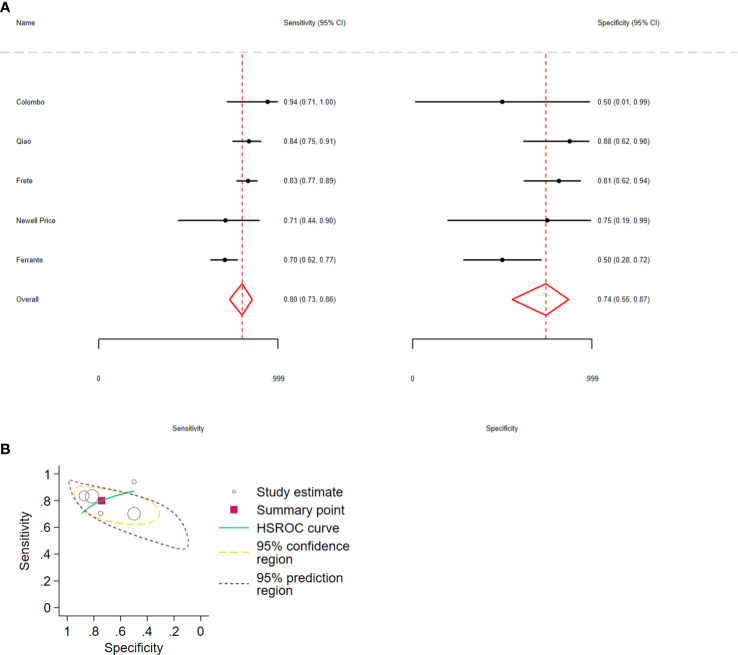
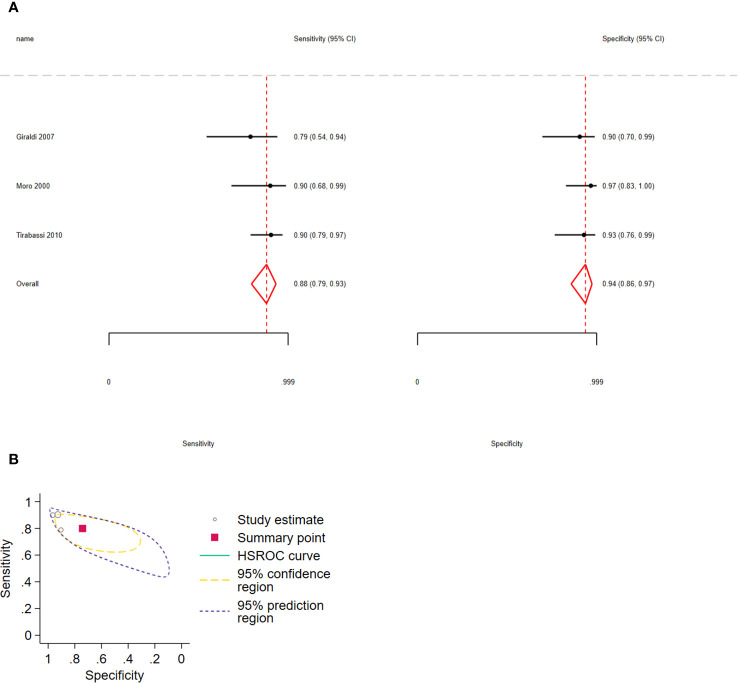
We evaluated the accuracy of the 10 μg desmopressin test in differentiating Cushing disease (CD) from non-neoplastic hypercortisolism (NNH) and ectopic ACTH syndrome (EAS). A systematic review of studies on diagnostic test accuracy in patients with CD, NNH, or EAS subjected to the desmopressin test obtained from LILACS, PubMed, EMBASE, and CENTRAL databases was performed. Two reviewers independently selected the studies, assessed the risk of bias, and extracted the data. Hierarchical and bivariate models on Stata software were used for meta-analytical summaries. The certainty of evidence was measured using the GRADE (Grading of Recommendations Assessment, Development, and Evaluation Working Group) approach. In total, 14 studies were included: 3 studies on differentiated CD versus NNH and 11 studies on differentiated CD versus EAS. Considering ΔACTH in 8 studies involving 429 patients, the pooled sensitivity for distinguishing CD from EAS was 0.85 (95% confidence interval [CI]: 0.80-0.89, I2 = 17.6%) and specificity was 0.64 (95% CI: 0.49-0.76, I2 = 9.46%). Regarding Δcortisol in 6 studies involving 233 participants, the sensitivity for distinguishing CD from EAS was 0.81 (95% CI: 0.74-0.87, I2 = 7.98%) and specificity was 0.80 (95% CI: 0.61-0.91, I2 = 12.89%). The sensitivity and specificity of the combination of ΔACTH > 35% and Δcortisol > 20% in 5 studies involving 511 participants were 0.88 (95% CI: 0.79-0.93, I2 = 35%) and 0.74 (95% CI: 0.55-0.87, I2 = 27%), respectively. The pooled sensitivity for distinguishing CD from NNH in 3 studies involving 170 participants was 0.88 (95% CI: 0.79-0.93) and the specificity was 0.94 (95% CI: 0.86-0.97). Based on the desmopressin test for differentiating CD from EAS, considering ΔACTH, Δcortisol, or both percent increments, 15%, 19%, or 20% of patients with CD, respectively, would be incorrectly classified as having EAS. For CD versus NNH, 11% of patients with CD would be falsely diagnosed as having NNH, whereas 7% of patients with NNH would be falsely diagnosed as having CD. However, in all hierarchical plots, the prediction intervals were considerably wider than the confidence intervals. This indicates low confidence in the estimated accuracy, and the true accuracy is likely to be different.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=85634, identifier CRD42018085634; https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=68317, identifier CRD42017068317.
Keywords: Cushing disease; Cushing syndrome; desmopressin test; non-neoplastic hypercortisolism; pseudo-Cushing syndrome; systematic review.
Copyright © 2024 Giampietro, Cabral, Pereira, Machado, Vilar and Nunes-Nogueira.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Dynamic Testing for Differential Diagnosis of ACTH-Dependent Cushing Syndrome: A Systematic Review and Meta-analysis.J Clin Endocrinol Metab. 2023 Apr 13;108(5):e178-e188. doi: 10.1210/clinem/dgac686. J Clin Endocrinol Metab. 2023. PMID: 36453141
-
The desmopressin and combined CRH-desmopressin tests in the differential diagnosis of ACTH-dependent Cushing's syndrome: constraints imposed by the expression of V2 vasopressin receptors in tumors with ectopic ACTH secretion.J Clin Endocrinol Metab. 2002 Apr;87(4):1646-53. doi: 10.1210/jcem.87.4.8358. J Clin Endocrinol Metab. 2002. PMID: 11932296
-
The limited value of the desmopressin test in the diagnostic approach to Cushing's syndrome.Clin Endocrinol (Oxf). 2001 May;54(5):609-16. doi: 10.1046/j.1365-2265.2001.01260.x. Clin Endocrinol (Oxf). 2001. PMID: 11380491
-
Enhancing Cushing's disease diagnosis: exploring the impact of desmopressin on ACTH gradient during BIPSS.Front Endocrinol (Lausanne). 2023 Aug 3;14:1224001. doi: 10.3389/fendo.2023.1224001. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37600715 Free PMC article.
-
Positive predictive value and trends of inferior petrosal sinus sampling (IPSS) in diagnosing cushing disease and ectopic ACTH secretion: A systematic review and meta-analysis.Clin Neurol Neurosurg. 2022 Sep;220:107350. doi: 10.1016/j.clineuro.2022.107350. Epub 2022 Jun 24. Clin Neurol Neurosurg. 2022. PMID: 35820339
Cited by
-
Differential diagnosis between Cushing's syndrome and non-neoplastic hypercortisolism: are we getting there?Pituitary. 2024 Oct;27(5):451-454. doi: 10.1007/s11102-024-01458-0. Epub 2024 Sep 19. Pituitary. 2024. PMID: 39298060 No abstract available.
References
-
- Findling JW, Raff H. DIAGNOSIS OF ENDOCRINE DISEASE: differentiation of pathologic/neoplastic hypercortisolism (Cushing’s syndrome) from physiologic/non-neoplastic hypercortisolism (formerly known as pseudo-Cushing’s syndrome). Eur J Endocrinol (2017) 176:R205–16. doi: 10.1530/EJE-16-0946 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical