

Case fatality and functional outcome after spontaneous subarachnoid haemorrhage: A systematic review and meta-analysis of time trends and regional variations in population-based studies
- PMID: 38353205
- PMCID: PMC11418425
- DOI: 10.1177/23969873241232823
Case fatality and functional outcome after spontaneous subarachnoid haemorrhage: A systematic review and meta-analysis of time trends and regional variations in population-based studies
Abstract
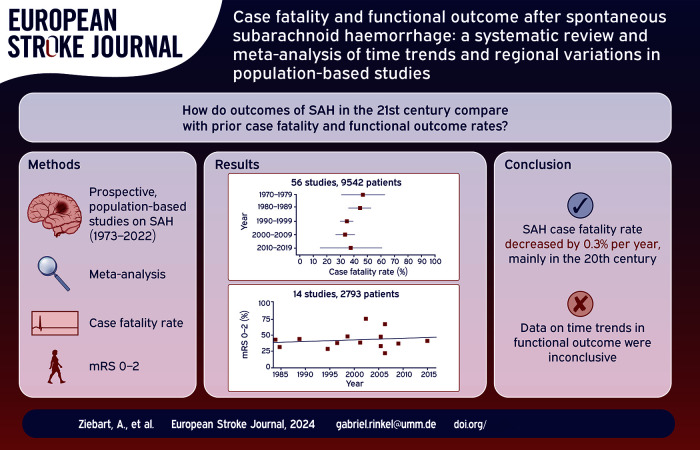
Introduction: A previous systematic review of population-based studies from 1973 to 2002 found a decrease in case fatality for spontaneous subarachnoid haemorrhage, but could not find a sufficient number of studies to assess changes in functional outcome. Since then, treatment has advanced distinctly. We assessed whether case fatality has decreased further and whether functional outcome has improved.
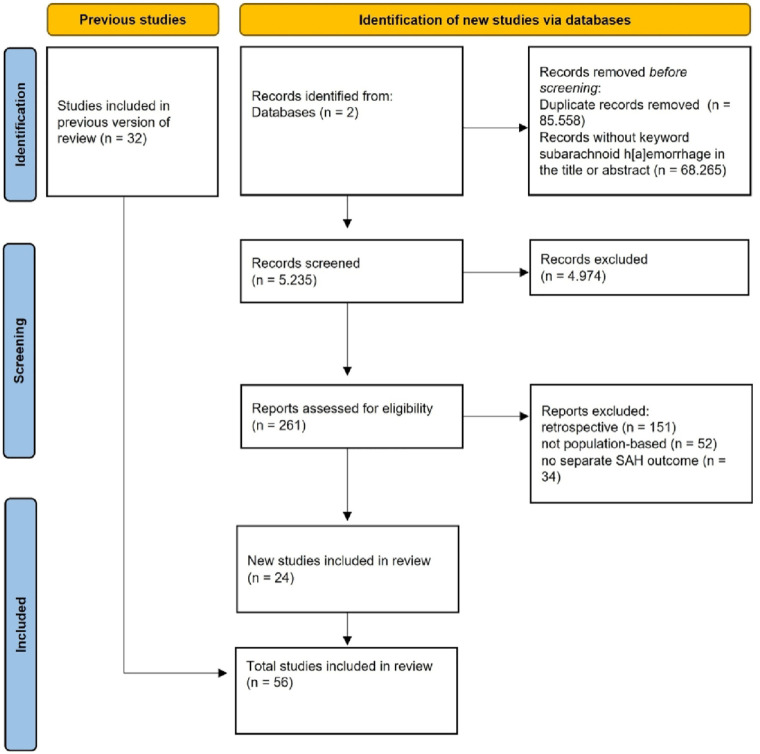
Patients and methods: We searched PubMed and Web of Science for new population-based studies using the same criteria as in our previous systematic review. We assessed changes in case fatality and functional outcome over time using linear regression.
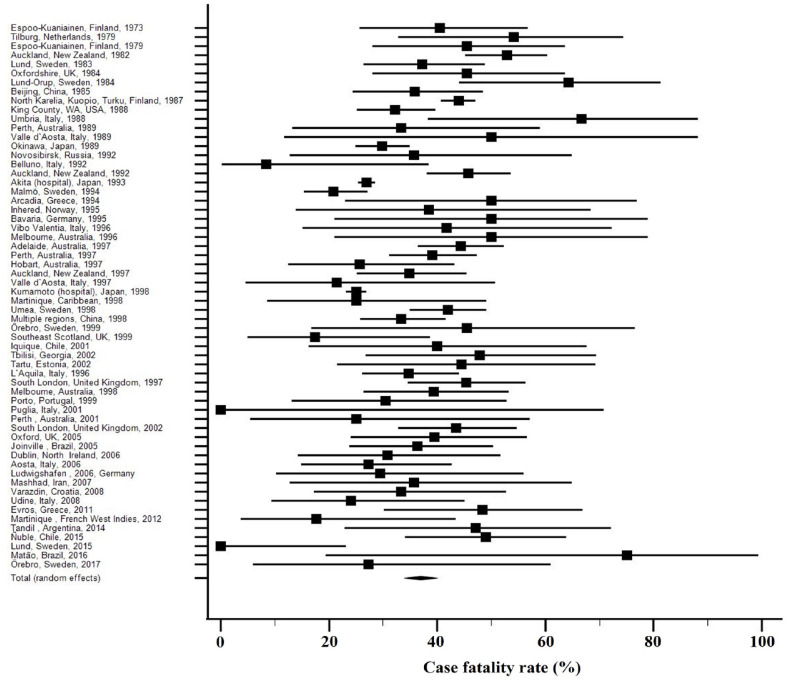
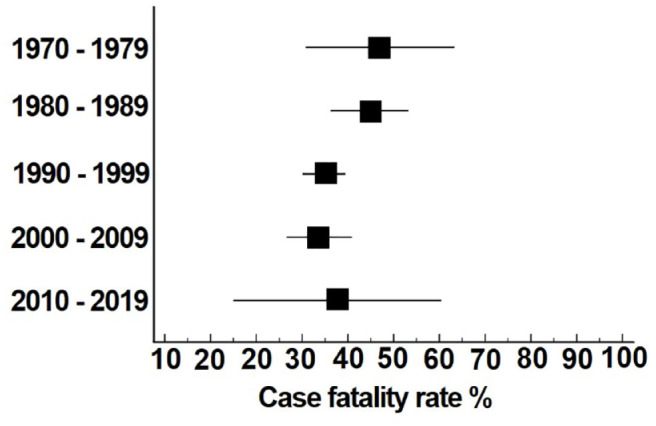
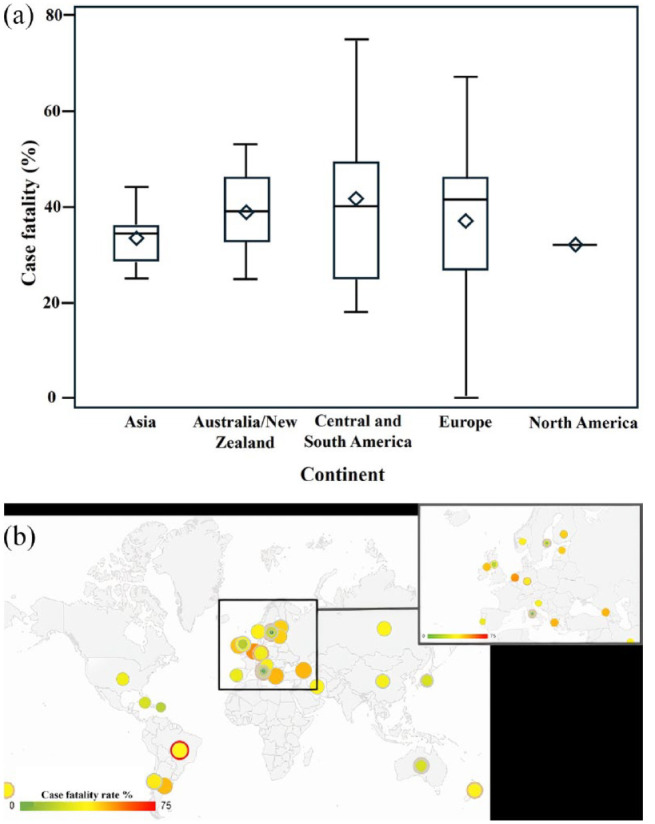
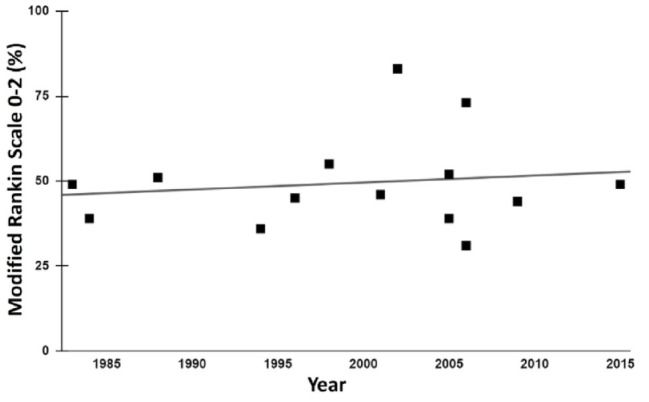
Results: We included 24 new studies with 827 patients and analysed 9542 patients described in 62 study periods between 1973 and 2017. Case fatality decreased by 0.3% (95% CI: -0.7 to 0.1) per year. In a sensitivity analysis excluding studies that did not provide 1-month outcome and outliers, the age and sex-adjusted decrease was 0.1% per year (95% CI: -0.9 to 0.6). The mean case fatality rate decreased from 47% (95% CI: 31-63) in the 1970s to 35% (95% CI: 30-39) in the 1990s, and remained stable in the 2000s (34%; 95% CI: 27-41) and 2010s (38%; 95% CI: 15-60). In 15 studies, the mean proportion of patients living independently increased by 0.2% per year (95%CI: -0.7 to 1.1) and the mean was 45% (95% CI: 39-50) in six studies that reported outcome after 12 months.
Discussion and conclusion: From 1973 to 2017, the case-fatality rate of spontaneous subarachnoid haemorrhage declined overall by 13.5%, but remained stable over the last two decades. The data on time trends in functional outcome were inconclusive.
Keywords: Subarachnoid haemorrhage; aneurysm; case fatality; functional outcome; stroke.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Nieuwkamp DJ, Setz LE, Algra A, et al. Changes in case fatality of aneurysmal subarachnoid haemorrhage over time, according to age, sex, and region: a meta-analysis. Lancet Neurol 2009; 8: 635–642. - PubMed
-
- Molyneux A, Kerr R, Stratton I, et al.; International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet 2002; 360: 1267–1274. - PubMed
-
- Lin N, Cahill KS, Frerichs KU, et al. Treatment of ruptured and unruptured cerebral aneurysms in the USA: a paradigm shift. J Neurointerv Surg 2018; 10: i69–i76. - PubMed
-
- SVIN COVID-19 Global SAH Registry. Global impact of the COVID-19 pandemic on subarachnoid haemorrhage hospitalisations, aneurysm treatment and in-hospital mortality: 1-year follow-up. J Neurol Neurosurg Psychiatry 2022; 93: 1028–1038. - PubMed
-
- Lindgren A, Burt S, Bragan Turner E, et al. Hospital case-volume is associated with case-fatality after aneurysmal subarachnoid hemorrhage. Int J Stroke 2019; 14: 282–289. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
