

Digital Health Interventions for Hypertension Management in US Populations Experiencing Health Disparities: A Systematic Review and Meta-Analysis
- PMID: 38353950
- PMCID: PMC10867699
- DOI: 10.1001/jamanetworkopen.2023.56070
Digital Health Interventions for Hypertension Management in US Populations Experiencing Health Disparities: A Systematic Review and Meta-Analysis
Abstract
Importance: Hypertension remains a leading factor associated with cardiovascular disease, and demographic and socioeconomic disparities in blood pressure (BP) control persist. While advances in digital health technologies have increased individuals' access to care for hypertension, few studies have analyzed the use of digital health interventions in vulnerable populations.
Objective: To assess the association between digital health interventions and changes in BP and to characterize tailored strategies for populations experiencing health disparities.
Data sources: In this systematic review and meta-analysis, a systematic search identified studies evaluating digital health interventions for BP management in the Cochrane Library, Ovid Embase, Google Scholar, Ovid MEDLINE, PubMed, Scopus, and Web of Science databases from inception until October 30, 2023.
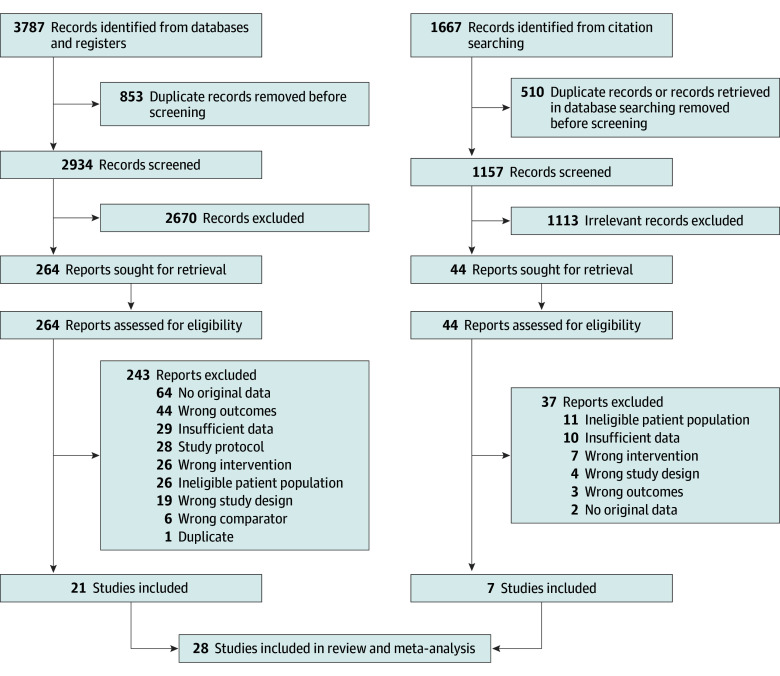
Study selection: Included studies were randomized clinical trials or cohort studies that investigated digital health interventions for managing hypertension in adults; presented change in systolic BP (SBP) or baseline and follow-up SBP levels; and emphasized social determinants of health and/or health disparities, including a focus on marginalized populations that have historically been underserved or digital health interventions that were culturally or linguistically tailored to a population with health disparities. The study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guideline.
Data extraction and synthesis: Two reviewers extracted and verified data. Mean differences in BP between treatment and control groups were analyzed using a random-effects model.
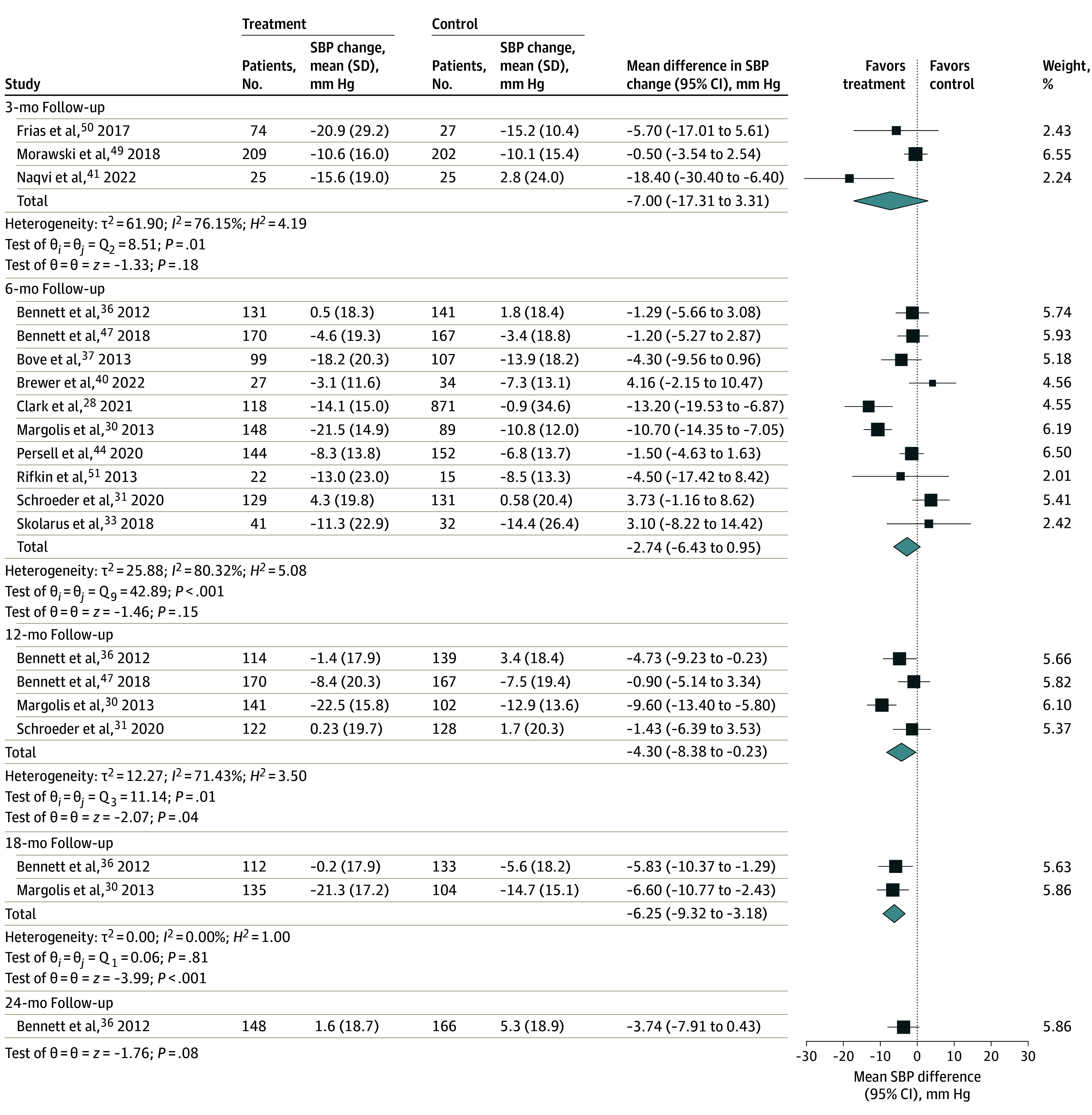
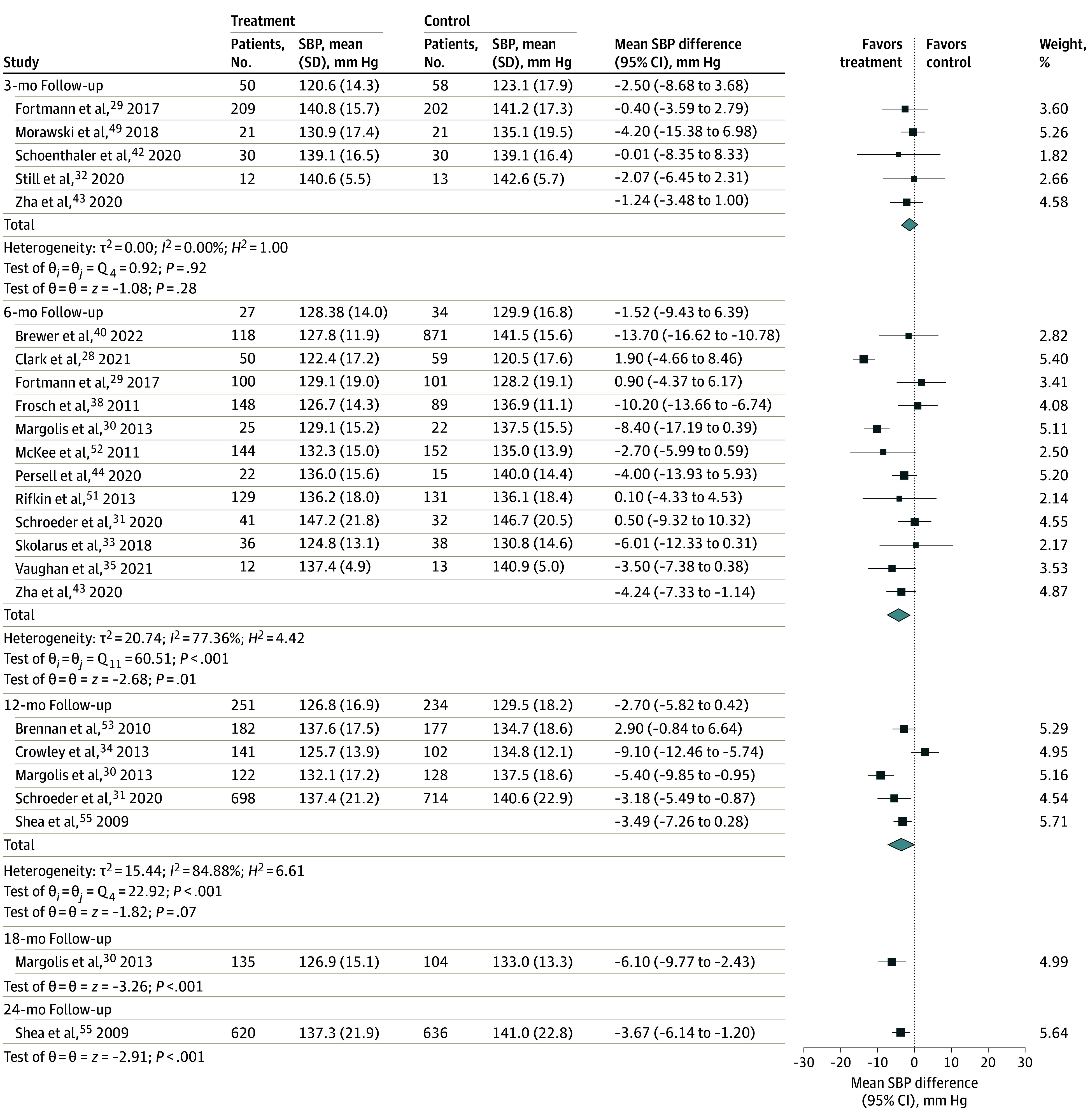
Main outcomes and measures: Primary outcomes included mean differences (95% CIs) in SBP and diastolic BP (DBP) from baseline to 6 and 12 months of follow-up between digital health intervention and control groups. Shorter- and longer-term follow-up durations were also assessed, and sensitivity analyses accounted for baseline BP levels.
Results: A total of 28 studies (representing 8257 participants) were included (overall mean participant age, 57.4 years [range, 46-71 years]; 4962 [60.1%], female). Most studies examined multicomponent digital health interventions incorporating remote BP monitoring (18 [64.3%]), community health workers or skilled nurses (13 [46.4%]), and/or cultural tailoring (21 [75.0%]). Sociodemographic characteristics were similar between intervention and control groups. Between the intervention and control groups, there were statistically significant mean differences in SBP at 6 months (-4.24 mm Hg; 95% CI, -7.33 to -1.14 mm Hg; P = .01) and SBP changes at 12 months (-4.30 mm Hg; 95% CI, -8.38 to -0.23 mm Hg; P = .04). Few studies (4 [14.3%]) reported BP changes and hypertension control beyond 1 year.
Conclusions and relevance: In this systematic review and meta-analysis of digital health interventions for hypertension management in populations experiencing health disparities, BP reductions were greater in the intervention groups compared with the standard care groups. The findings suggest that tailored initiatives that leverage digital health may have the potential to advance equity in hypertension outcomes.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
