

Zinpentraxin Alfa for Idiopathic Pulmonary Fibrosis: The Randomized Phase III STARSCAPE Trial
- PMID: 38354066
- PMCID: PMC11092957
- DOI: 10.1164/rccm.202401-0116OC
Zinpentraxin Alfa for Idiopathic Pulmonary Fibrosis: The Randomized Phase III STARSCAPE Trial
Abstract
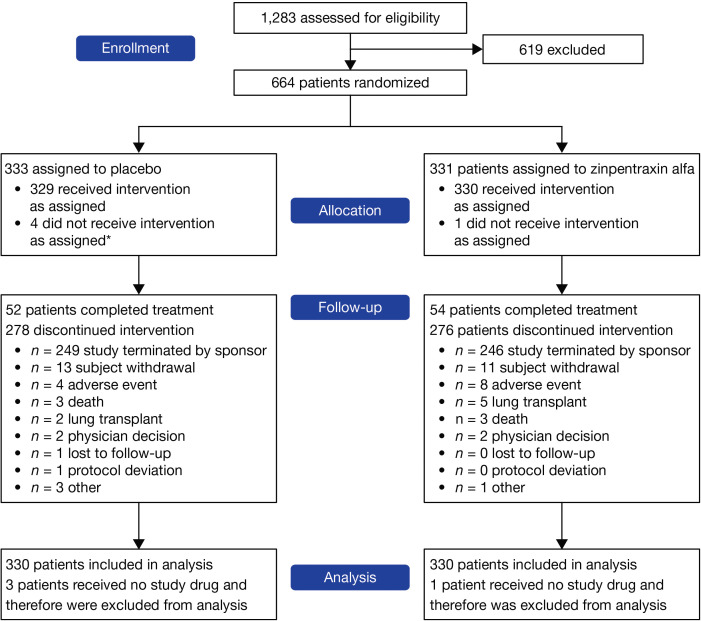
Rationale: A phase II trial reported clinical benefit over 28 weeks in patients with idiopathic pulmonary fibrosis (IPF) who received zinpentraxin alfa. Objectives: To investigate the efficacy and safety of zinpentraxin alfa in patients with IPF in a phase III trial. Methods: This 52-week phase III, double-blind, placebo-controlled, pivotal trial was conducted at 275 sites in 29 countries. Patients with IPF were randomized 1:1 to intravenous placebo or zinpentraxin alfa 10 mg/kg every 4 weeks. The primary endpoint was absolute change from baseline to Week 52 in FVC. Secondary endpoints included absolute change from baseline to Week 52 in percent predicted FVC and 6-minute walk distance. Safety was monitored via adverse events. Post hoc analysis of the phase II and phase III data explored changes in FVC and their impact on the efficacy results. Measurements and Main Results: Of 664 randomized patients, 333 were assigned to placebo and 331 to zinpentraxin alfa. Four of the 664 randomized patients were never administered study drug. The trial was terminated early after a prespecified futility analysis that demonstrated no treatment benefit of zinpentraxin alfa over placebo. In the final analysis, absolute change from baseline to Week 52 in FVC was similar between placebo and zinpentraxin alfa (-214.89 ml and -235.72 ml; P = 0.5420); there were no apparent treatment effects on secondary endpoints. Overall, 72.3% and 74.6% of patients receiving placebo and zinpentraxin alfa, respectively, experienced one or more adverse events. Post hoc analysis revealed that extreme FVC decline in two placebo-treated patients resulted in the clinical benefit of zinpentraxin alfa reported by phase II. Conclusions: Zinpentraxin alfa treatment did not benefit patients with IPF over placebo. Learnings from this program may help improve decision making around trials in IPF. Clinical trial registered with www.clinicaltrials.gov (NCT04552899).
Keywords: antifibrotic medication; forced vital capacity; futility analysis; interstitial lung disease; linear mixed-effects model.
Figures


Comment in
-
Advancing Drug Development in Idiopathic Pulmonary Fibrosis: Tomorrow Is Now.Am J Respir Crit Care Med. 2024 May 1;209(9):1060-1062. doi: 10.1164/rccm.202402-0381ED. Am J Respir Crit Care Med. 2024. PMID: 38484134 Free PMC article. No abstract available.
References
-
- Raghu G, Remy-Jardin M, Myers JL, Richeldi L, Ryerson CJ, Lederer DJ, et al. American Thoracic Society, European Respiratory Society, Japanese Respiratory Society, and Latin American Thoracic Society Diagnosis of idiopathic pulmonary fibrosis: an official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med . 2018;198:e44–e68. - PubMed
-
- Cottin V, Tomassetti S, Valenzuela C, Walsh SLF, Antoniou KM, Bonella F, et al. Integrating clinical probability into the diagnostic approach to idiopathic pulmonary fibrosis: an International Working Group perspective. Am J Respir Crit Care Med . 2022;206:247–259. - PubMed
-
- Richeldi L, du Bois RM, Raghu G, Azuma A, Brown KK, Costabel U, et al. INPULSIS Trial Investigators Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N Engl J Med . 2014;370:2071–2082. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
