

Incorporating frailty to address the key challenges to geriatric economic evaluation
- PMID: 38355461
- PMCID: PMC10868084
- DOI: 10.1186/s12877-024-04752-5
Incorporating frailty to address the key challenges to geriatric economic evaluation
Abstract
Background: The multidimensional and dynamically complex process of ageing presents key challenges to economic evaluation of geriatric interventions, including: (1) accounting for indirect, long-term effects of a geriatric shock such as a fall; (2) incorporating a wide range of societal, non-health outcomes such as informal caregiver burden; and (3) accounting for heterogeneity within the demographic group. Measures of frailty aim to capture the multidimensional and syndromic nature of geriatric health. Using a case study of community-based falls prevention, this article explores how incorporating a multivariate frailty index in a decision model can help address the above key challenges.
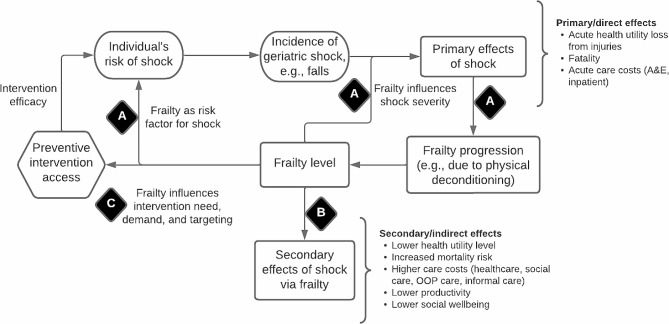
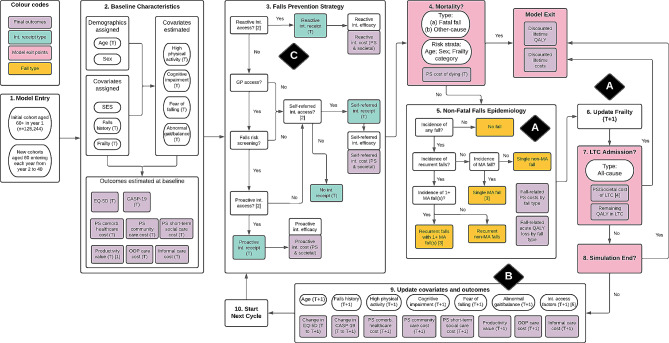
Methods: A conceptual structure of the relationship between geriatric shocks and frailty was developed. This included three key associations involving frailty: (A) the shock-frailty feedback loop; (B) the secondary effects of shock via frailty; and (C) association between frailty and intervention access. A case study of economic modelling of community-based falls prevention for older persons aged 60 + was used to show how parameterising these associations contributed to addressing the above three challenges. The English Longitudinal Study of Ageing (ELSA) was the main data source for parameterisation. A new 52-item multivariate frailty index was generated from ELSA. The main statistical methods were multivariate logistic and linear regressions. Estimated regression coefficients were inputted into a discrete individual simulation with annual cycles to calculate the continuous variable value or probability of binary event given individuals' characteristics.
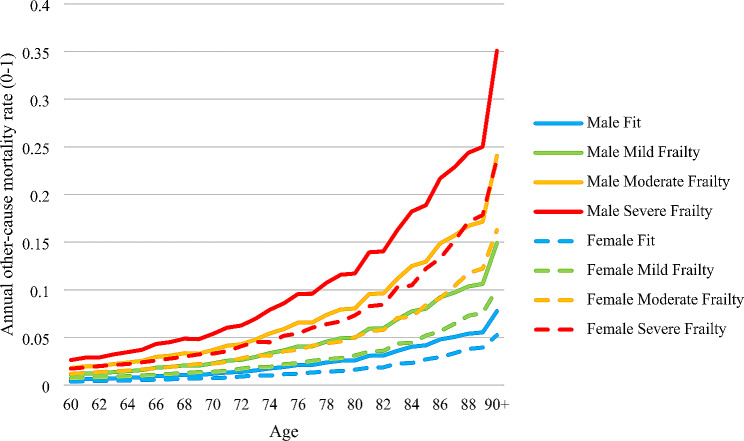
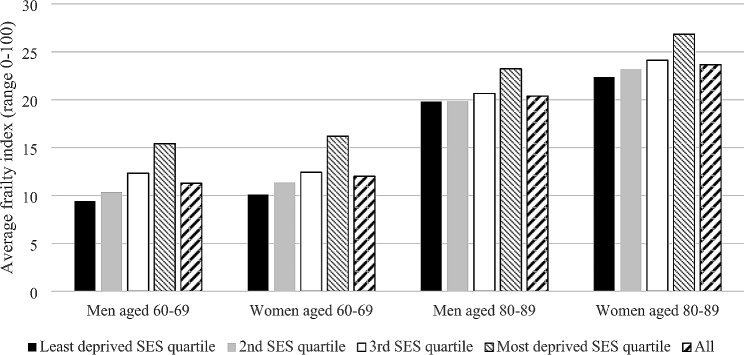
Results: All three conceptual associations, in their parameterised forms, contributed to addressing challenge (1). Specifically, by worsening the frailty progression, falls incidence in the model increased the risk of falling in subsequent cycles and indirectly impacted the trajectories and levels of EQ-5D-3 L, mortality risk, and comorbidity care costs. Intervention access was positively associated with frailty such that the greater access to falls prevention by frailer individuals dampened the falls-frailty feedback loop. Association (B) concerning the secondary effects of falls via frailty was central to addressing challenge (2). Using this association, the model was able to estimate how falls prevention generated via its impact on frailty paid and unpaid productivity gains, out-of-pocket care expenditure reduction, and informal caregiving cost reduction. For challenge (3), frailty captured the variations within demographic groups of key model outcomes including EQ-5D-3 L, QALY, and all-cause care costs. Frailty itself was shown to have a social gradient such that it mediated socially inequitable distributions of frailty-associated outcomes.
Conclusion: The frailty-based conceptual structure and parameterisation methods significantly improved upon the methods previously employed by falls prevention models to address the key challenges for geriatric economic evaluation. The conceptual structure is applicable to other geriatric and non-geriatric intervention areas and should inform the data selection and statistical methods to parameterise structurally valid economic models of geriatric interventions.
Keywords: Economic model; Equity; Falls prevention; Frailty; Long-term outcomes; Societal outcomes.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organization. World Report on Ageing and Health. World Health Organization; 2015.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
