

Characteristics and outcomes of patients with do-not-resuscitate and physician orders for life-sustaining treatment in a medical intensive care unit: a retrospective cohort study
- PMID: 38355511
- PMCID: PMC10868112
- DOI: 10.1186/s12904-024-01375-w
Characteristics and outcomes of patients with do-not-resuscitate and physician orders for life-sustaining treatment in a medical intensive care unit: a retrospective cohort study
Abstract
Background: In the intensive care unit (ICU), we may encounter patients who have completed a Do-Not-Resuscitate (DNR) or a Physician Orders to Stop Life-Sustaining Treatment (POLST) document. However, the characteristics of ICU patients who choose DNR/POLST are not well understood.
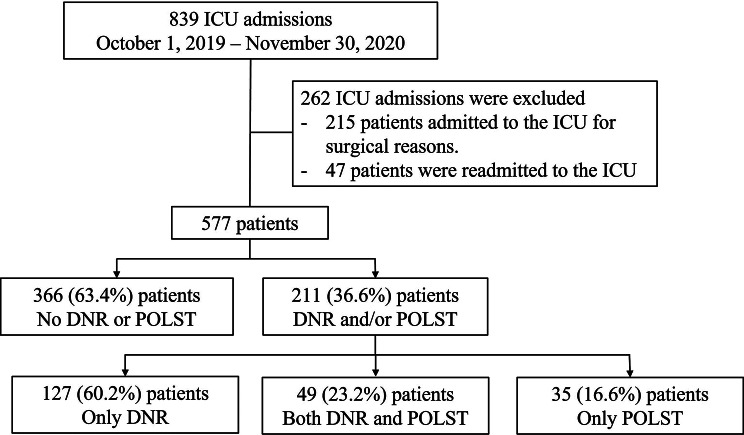
Methods: We retrospectively analyzed the electronic medical records of 577 patients admitted to a medical ICU from October 2019 to November 2020, focusing on the characteristics of patients according to whether they completed DNR/POLST documents. Patients were categorized into DNR/POLST group and no DNR/POLST group according to whether they completed DNR/POLST documents, and logistic regression analysis was used to evaluate factors influencing DNR/POLST document completion.
Results: A total of 577 patients were admitted to the ICU. Of these, 211 patients (36.6%) had DNR or POLST records. DNR and/or POLST were completed prior to ICU admission in 48 (22.7%) patients. The DNR/POLST group was older (72.9 ± 13.5 vs. 67.6 ± 13.8 years, p < 0.001) and had higher Acute Physiology and Chronic Health Evaluation (APACHE) II score (26.1 ± 9.2 vs. 20.3 ± 7.7, p < 0.001) and clinical frailty scale (5.1 ± 1.4 vs. 4.4 ± 1.4, p < 0.001) than the other groups. Solid tumors, hematologic malignancies, and chronic lung disease were the most common comorbidities in the DNR/POLST groups. The DNR/POLST group had higher ICU and in-hospital mortality and more invasive treatments (arterial line, central line, renal replacement therapy, invasive mechanical ventilation) than the other groups. Body mass index, APAHCE II score, hematologic malignancy, DNR/POLST were factors associated with in-hospital mortality.
Conclusions: Among ICU patients, 36.6% had DNR or POLST orders and received more invasive treatments. This is contrary to the common belief that DNR/POLST patients would receive less invasive treatment and underscores the need to better understand and include end-of-life care as an important ongoing aspect of patient care, along with communication with patients and families.
Keywords: Do not resuscitate; Life-sustaining treatment; Medical treatment; Risk factors.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Won YW, Kim HJ, Kwon JH, Lee HY, Baek SK, Kim YJ, Kim DY, Ryu H. Life-sustaining Treatment States in Korean Cancer patients after Enforcement of Act on decisions on life-sustaining treatment for patients at the end of life. Cancer Res Treat. 2021;53(4):908–16. doi: 10.4143/crt.2021.325. - DOI - PMC - PubMed
-
- Chang YC, Fang YT, Chen HC, Lin CY, Chang YP, Chen YM, Huang CH, Huang KT, Chang HC, Su MC, et al. Effect of do-not-resuscitate orders on patients with sepsis in the medical intensive care unit: a retrospective, observational and propensity score-matched study in a tertiary referral hospital in Taiwan. BMJ open. 2019;9(6):e029041. doi: 10.1136/bmjopen-2019-029041. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
