

Development and validation of a prospective study to predict the risk of readmission within 365 days of respiratory failure: based on a random survival forest algorithm combined with COX regression modeling
- PMID: 38355552
- PMCID: PMC10865688
- DOI: 10.1186/s12890-024-02862-9
Development and validation of a prospective study to predict the risk of readmission within 365 days of respiratory failure: based on a random survival forest algorithm combined with COX regression modeling
Abstract
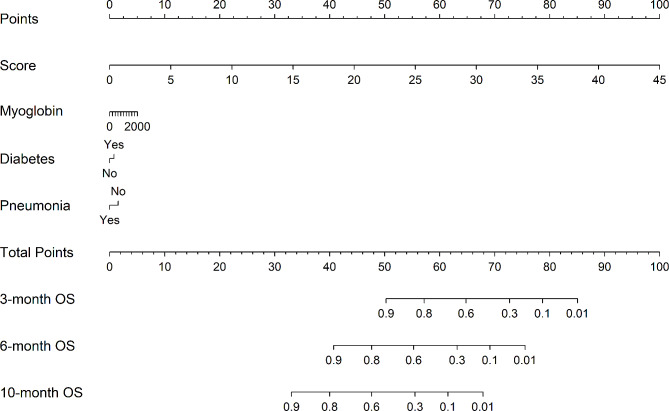
Background: There is a need to develop and validate a widely applicable nomogram for predicting readmission of respiratory failure patients within 365 days.
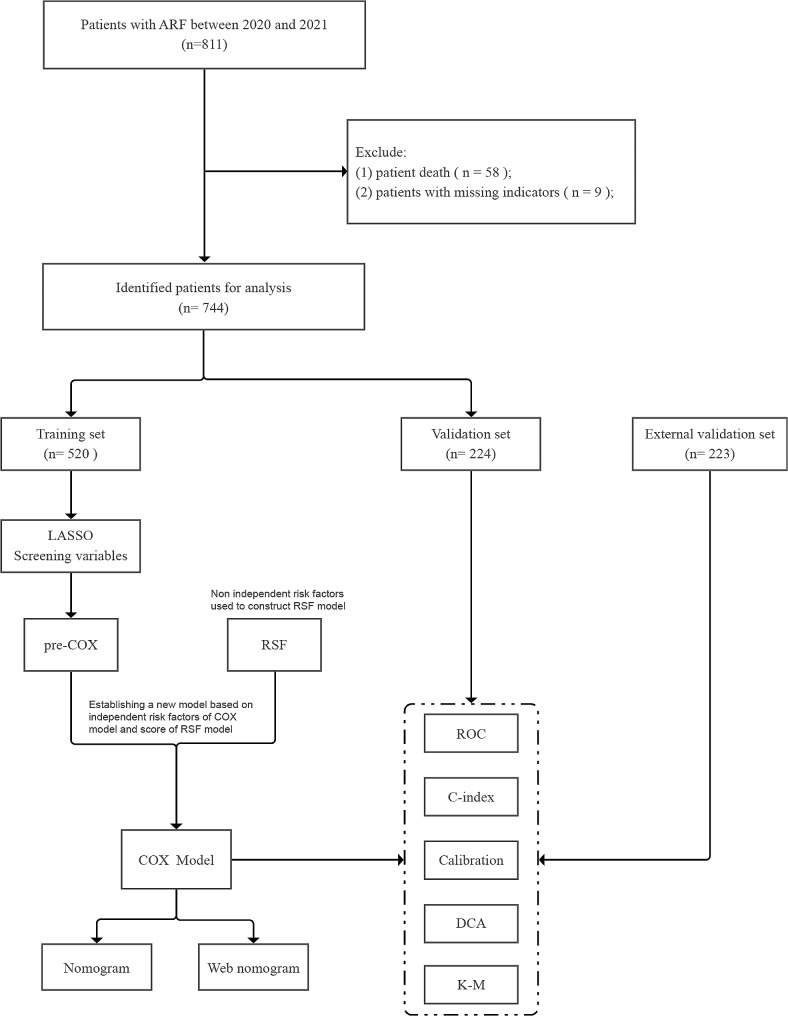
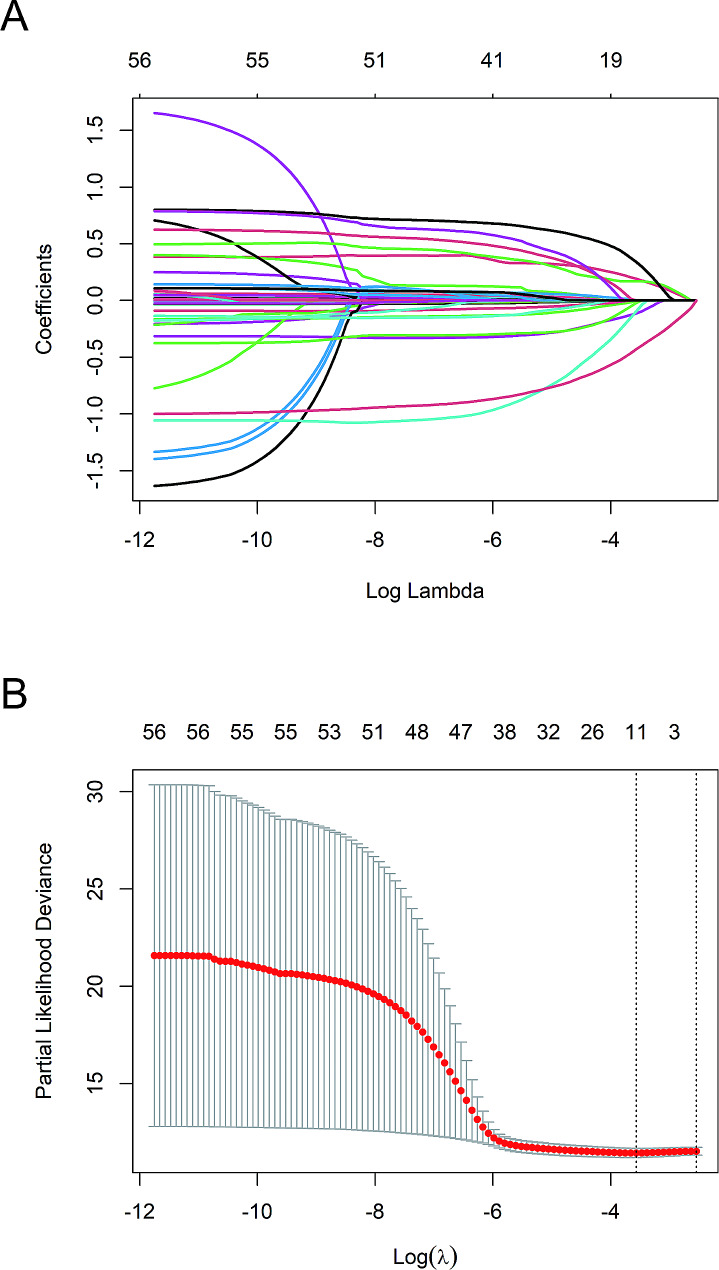
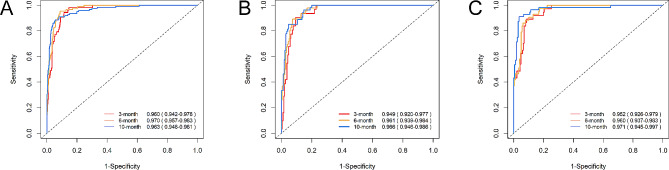
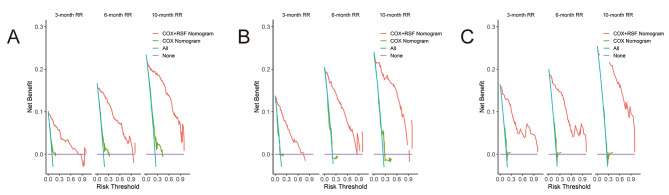
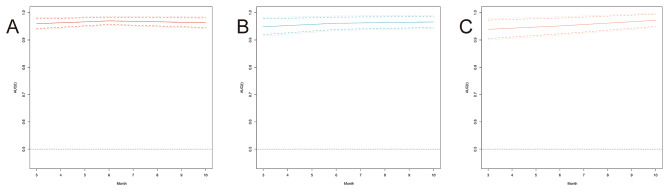
Methods: We recruited patients with respiratory failure at the First People's Hospital of Yancheng and the People's Hospital of Jiangsu. We used the least absolute shrinkage and selection operator regression to select significant features for multivariate Cox proportional hazard analysis. The Random Survival Forest algorithm was employed to construct a model for the variables that obtained a coefficient of 0 following LASSO regression, and subsequently determine the prediction score. Independent risk factors and the score were used to develop a multivariate COX regression for creating the line graph. We used the Harrell concordance index to quantify the predictive accuracy and the receiver operating characteristic curve to evaluate model performance. Additionally, we used decision curve analysiso assess clinical usefulness.
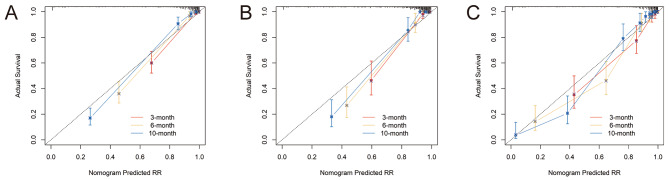
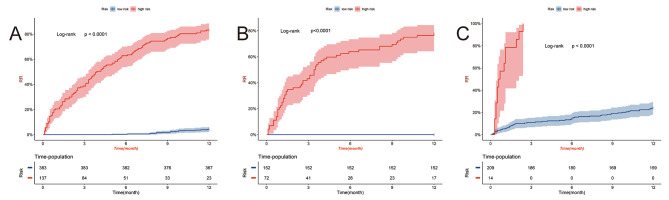
Results: The LASSO regression and multivariate Cox regression were used to screen hemoglobin, diabetes and pneumonia as risk variables combined with Score to develop a column chart model. The C index is 0.927 in the development queue, 0.924 in the internal validation queue, and 0.922 in the external validation queue. At the same time, the predictive model also showed excellent calibration and higher clinical value.
Conclusions: A nomogram predicting readmission of patients with respiratory failure within 365 days based on three independent risk factors and a jointly developed random survival forest algorithm has been developed and validated. This improves the accuracy of predicting patient readmission and provides practical information for individualized treatment decisions.
Keywords: COX regression modeling; Nomogram; Random survival forest algorithm; Readmission; Respiratory failure.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
