

Construction and validation of a predictive model of invasive adenocarcinoma in pure ground-glass nodules less than 2 cm in diameter
- PMID: 38355554
- PMCID: PMC10868041
- DOI: 10.1186/s12893-024-02341-2
Construction and validation of a predictive model of invasive adenocarcinoma in pure ground-glass nodules less than 2 cm in diameter
Abstract
Objectives: In this study, we aimed to develop a multiparameter prediction model to improve the diagnostic accuracy of invasive adenocarcinoma in pulmonary pure glass nodules.
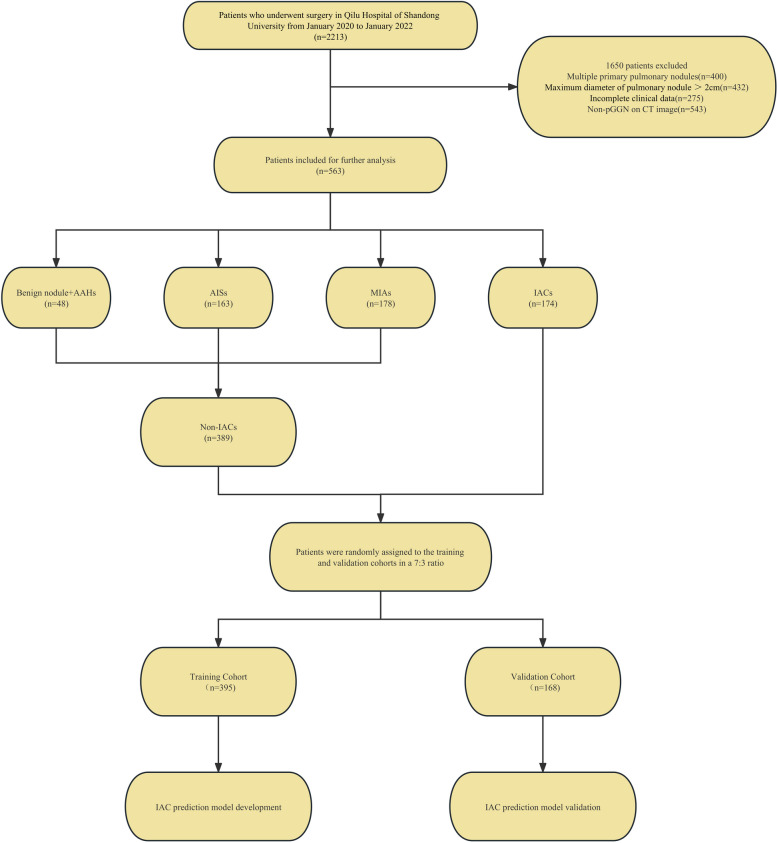
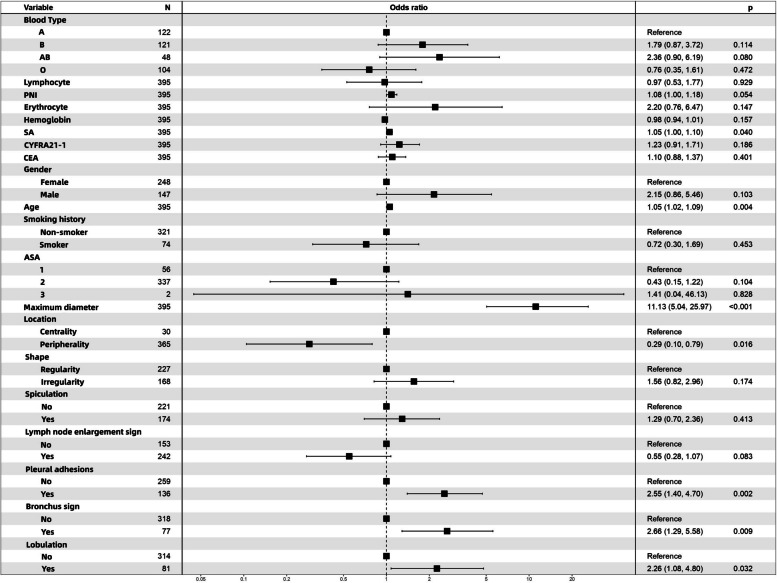
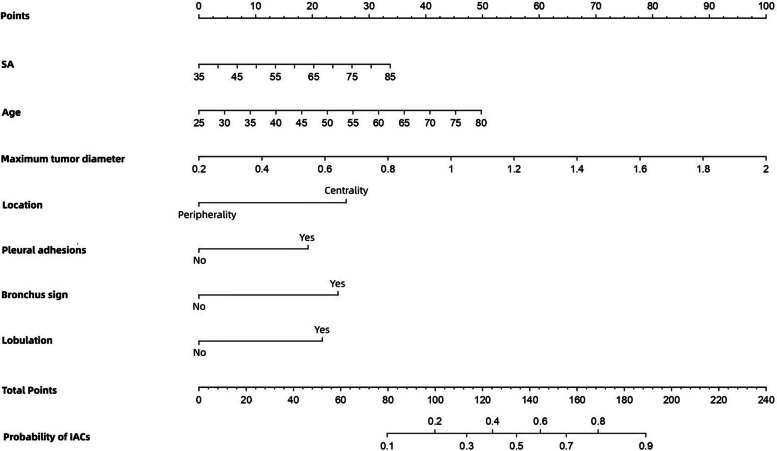
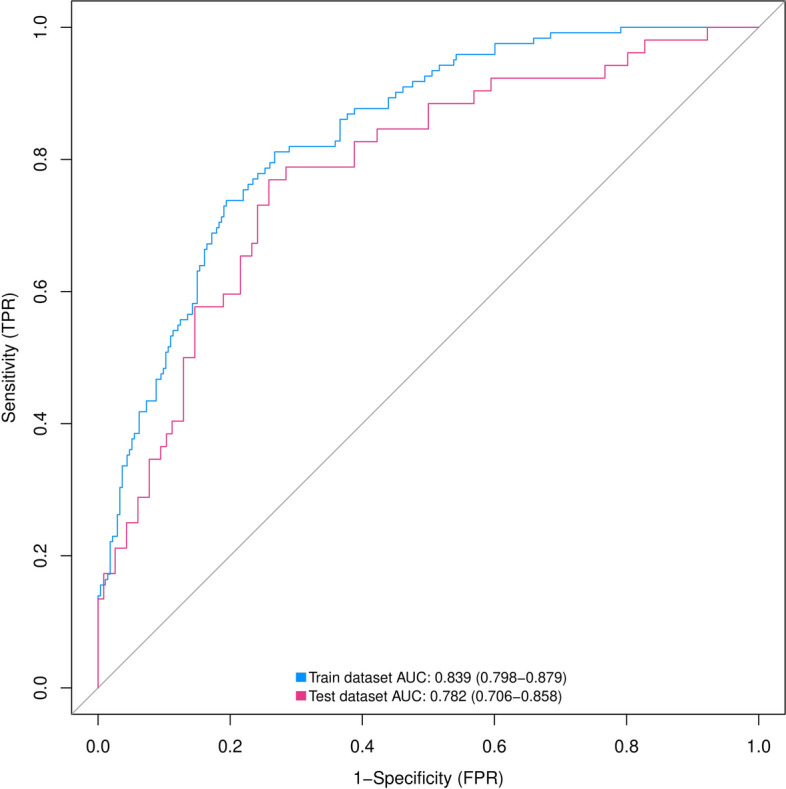
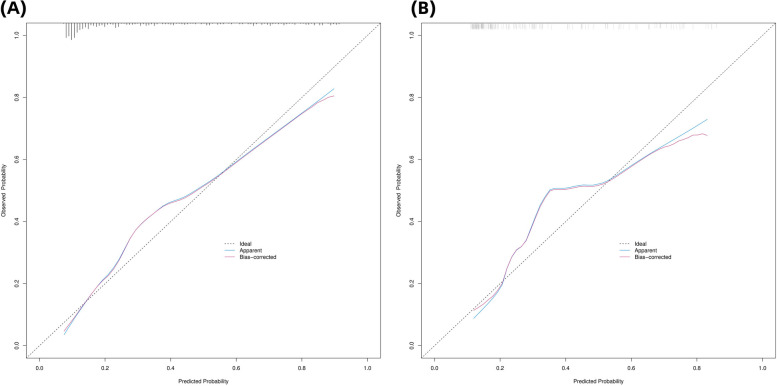
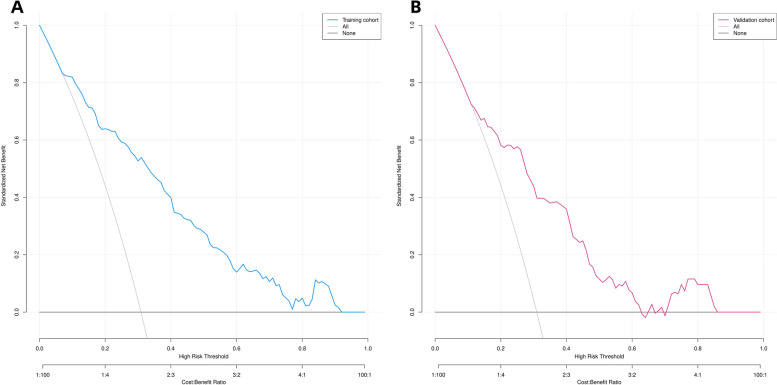
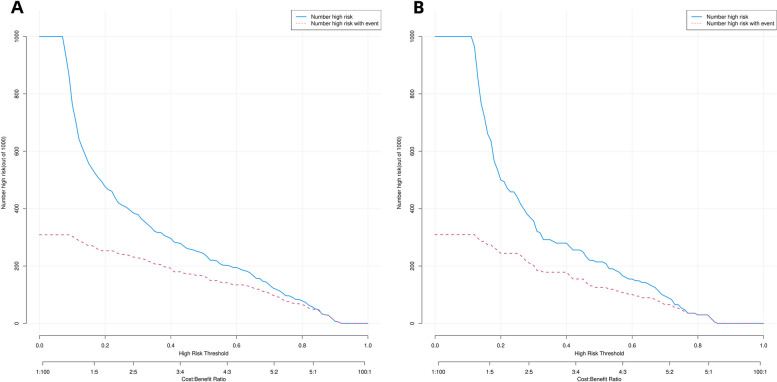
Method: We included patients with pulmonary pure glass nodules who underwent lung resection and had a clear pathology between January 2020 and January 2022 at the Qilu Hospital of Shandong University. We collected data on the clinical characteristics of the patients as well as their preoperative biomarker results and computed tomography features. Thereafter, we performed univariate and multivariate logistic regression analyses to identify independent risk factors, which were then used to develop a prediction model and nomogram. We then evaluated the recognition ability of the model via receiver operating characteristic (ROC) curve analysis and assessed its calibration ability using the Hosmer-Lemeshow test and calibration curves. Further, to assess the clinical utility of the nomogram, we performed decision curve analysis.
Result: We included 563 patients, comprising 174 and 389 cases of invasive and non-invasive adenocarcinoma, respectively, and identified seven independent risk factors, namely, maximum tumor diameter, age, serum amyloid level, pleural effusion sign, bronchial sign, tumor location, and lobulation. The area under the ROC curve was 0.839 (95% CI: 0.798-0.879) for the training cohort and 0.782 (95% CI: 0.706-0.858) for the validation cohort, indicating a relatively high predictive accuracy for the nomogram. Calibration curves for the prediction model also showed good calibration for both cohorts, and decision curve analysis showed that the clinical prediction model has clinical utility.
Conclusion: The novel nomogram thus constructed for identifying invasive adenocarcinoma in patients with isolated pulmonary pure glass nodules exhibited excellent discriminatory power, calibration capacity, and clinical utility.
Keywords: Invasive adenocarcinoma; Logical model; Nomogram; Prediction; Pulmonary pure glass nodule.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Nomogram for Predicting the Risk of Invasive Pulmonary Adenocarcinoma for Pure Ground-Glass Nodules.Ann Thorac Surg. 2018 Apr;105(4):1058-1064. doi: 10.1016/j.athoracsur.2017.11.012. Epub 2018 Feb 14. Ann Thorac Surg. 2018. PMID: 29452996
-
The role of adenocarcinoma subtypes and immunohistochemistry in predicting lymph node metastasis in early invasive lung adenocarcinoma.BMC Cancer. 2024 Jan 29;24(1):139. doi: 10.1186/s12885-024-11843-4. BMC Cancer. 2024. PMID: 38287300 Free PMC article.
-
Nomogram for predicting invasive lung adenocarcinoma in small solitary pulmonary nodules.Front Oncol. 2024 Jul 1;14:1334504. doi: 10.3389/fonc.2024.1334504. eCollection 2024. Front Oncol. 2024. PMID: 39011482 Free PMC article.
-
Development and validation of a risk prediction model for invasiveness of pure ground-glass nodules based on a systematic review and meta-analysis.BMC Med Imaging. 2024 Jun 17;24(1):149. doi: 10.1186/s12880-024-01313-5. BMC Med Imaging. 2024. PMID: 38886695 Free PMC article.
-
The infiltration risk prediction models by logistic regression for ground-glass pulmonary nodules: a systematic review and meta-analysis.Front Oncol. 2025 Jan 29;14:1477730. doi: 10.3389/fonc.2024.1477730. eCollection 2024. Front Oncol. 2025. PMID: 39943992 Free PMC article.
Cited by
-
Risk factors for the growth of ground-glass nodules in the lungs: A systematic review and meta-analysis.Clinics (Sao Paulo). 2025 May 7;80:100669. doi: 10.1016/j.clinsp.2025.100669. eCollection 2025. Clinics (Sao Paulo). 2025. PMID: 40339350 Free PMC article.
References
-
- Wu FZ, Huang YL, Wu CC, Tang EK, Chen CS, Mar GY, et al. Assessment of Selection Criteria for low-dose lung screening CT among Asian ethnic groups in Taiwan: from Mass Screening to specific risk-based screening for Non-smoker Lung Cancer. Clin Lung Cancer. 2016;17(5):e45–e56. doi: 10.1016/j.cllc.2016.03.004. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
