

Prevalence, regional distribution, and trends of antimicrobial resistance among female outpatients with urine Klebsiella spp. isolates: a multicenter evaluation in the United States between 2011 and 2019
- PMID: 38355621
- PMCID: PMC10865585
- DOI: 10.1186/s13756-024-01372-x
Prevalence, regional distribution, and trends of antimicrobial resistance among female outpatients with urine Klebsiella spp. isolates: a multicenter evaluation in the United States between 2011 and 2019
Abstract
Background: Antimicrobial resistance research in uncomplicated urinary tract infection typically focuses on the main causative pathogen, Escherichia coli; however, little is known about the antimicrobial resistance burden of Klebsiella species, which can also cause uncomplicated urinary tract infections. This retrospective cohort study assessed the prevalence and geographic distribution of antimicrobial resistance among Klebsiella species and antimicrobial resistance trends for K. pneumoniae in the United States (2011-2019).
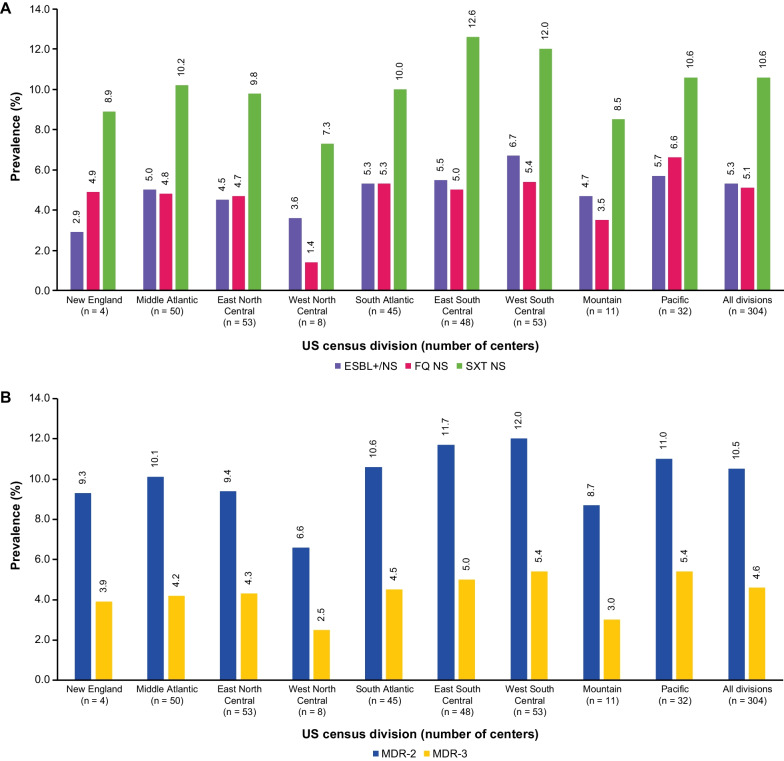
Methods: K. pneumoniae and K. oxytoca urine isolates (30-day, non-duplicate) among female outpatients (aged ≥ 12 years) with presumed uUTI at 304 centers in the United States were classified by resistance phenotype(s): not susceptible to nitrofurantoin, trimethoprim/sulfamethoxazole, or fluoroquinolone, extended-spectrum β-lactamase-positive/not susceptible; and multidrug-resistant based on ≥ 2 and ≥ 3 resistance phenotypes. Antimicrobial resistance prevalence by census division and age, as well as antimicrobial resistance trends over time for Klebsiella species, were assessed using generalized estimating equations.
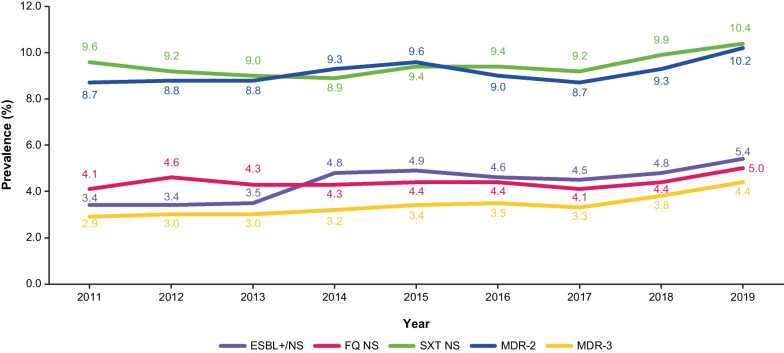
Results: 270,552 Klebsiella species isolates were evaluated (250,719 K. pneumoniae; 19,833 K. oxytoca). The most frequent resistance phenotypes in 2019 were nitrofurantoin not susceptible (Klebsiella species: 54.0%; K. pneumoniae: 57.3%; K. oxytoca: 15.1%) and trimethoprim/sulfamethoxazole not susceptible (Klebsiella species: 10.4%; K. pneumoniae: 10.6%; K. oxytoca: 8.6%). Extended-spectrum β-lactamase-positive/not susceptible prevalence was 5.4%, 5.3%, and 6.8%, respectively. K. pneumoniae resistance phenotype prevalence varied (p < 0.0001) geographically and by age, and increased over time (except for the nitrofurantoin not susceptible phenotype, which was stable and > 50% throughout).
Conclusions: There is a high antimicrobial resistance prevalence and increasing antimicrobial resistance trends among K. pneumoniae isolates from female outpatients in the United States with presumed uncomplicated urinary tract infection. Awareness of K. pneumoniae antimicrobial resistance helps to optimize empiric uncomplicated urinary tract infection treatment.
Keywords: Antimicrobial resistance; Klebsiella oxytoca; Klebsiella pneumoniae; Uncomplicated urinary tract infection.
© 2024. The Author(s).
Conflict of interest statement
KSK declares the following: consulting fees from AbbVie, Allecra, Carb-X, Merck, Shionogi, Spero, and Venatorx; and symposia honoraria from GSK. VG was an employee of, and shareholder in, Becton, Dickinson and Company at the time of the analysis, and the company received funding from GSK to conduct this study. AM is an employee of, and shareholder in, GSK. AVJ is an employee of, and shareholder in, GSK. GY was an employee of Becton, Dickinson and Company, and the company received funding from GSK to conduct this study. NESO is an employee of, and shareholder in, GSK. KY is an employee of, and shareholder in, Becton, Dickinson and Company, and the company received funding from GSK to conduct this study. FSMG is an employee of, and shareholder in, GSK. Some of the material discussed in this manuscript was previously presented at Infectious Diseases Week (IDWeek) 2022; Kaye, et al., presentation 2227, “Prevalence, Regional Distribution, and Trends of Antimicrobial Resistance Among Female Outpatients With Urine
Figures
Similar articles
-
Antimicrobial Resistance Trends in Urine Escherichia coli Isolates From Adult and Adolescent Females in the United States From 2011 to 2019: Rising ESBL Strains and Impact on Patient Management.Clin Infect Dis. 2021 Dec 6;73(11):1992-1999. doi: 10.1093/cid/ciab560. Clin Infect Dis. 2021. PMID: 34143881 Free PMC article.
-
A multicenter analysis of trends in resistance in urinary Enterobacterales isolates from ambulatory patients in the United States: 2011-2020.BMC Infect Dis. 2022 Feb 28;22(1):194. doi: 10.1186/s12879-022-07167-y. BMC Infect Dis. 2022. PMID: 35227203 Free PMC article.
-
Co-resistance Among Escherichia coli and Klebsiella pneumoniae Urine Isolates from Female Outpatients with Presumed UTI: A Retrospective US Cohort Study.Infect Dis Ther. 2024 Jul;13(7):1715-1722. doi: 10.1007/s40121-024-00995-2. Epub 2024 Jun 6. Infect Dis Ther. 2024. PMID: 38842759 Free PMC article.
-
Sulopenem: An Intravenous and Oral Penem for the Treatment of Urinary Tract Infections Due to Multidrug-Resistant Bacteria.Drugs. 2022 Apr;82(5):533-557. doi: 10.1007/s40265-022-01688-1. Epub 2022 Mar 16. Drugs. 2022. PMID: 35294769 Review.
-
Uncomplicated urinary tract infection in women. Current practice and the effect of antibiotic resistance on empiric treatment.Can Fam Physician. 2006 May;52(5):612-8. Can Fam Physician. 2006. PMID: 16739835 Free PMC article. Review.
Cited by
-
Associations between neighbourhood-level median household income and outpatients' risk of antibiotic non-susceptible uropathogens in a major urban centre, USA.JAC Antimicrob Resist. 2024 Nov 5;6(6):dlae179. doi: 10.1093/jacamr/dlae179. eCollection 2024 Dec. JAC Antimicrob Resist. 2024. PMID: 39502742 Free PMC article.
-
Major Predominant Serotypes and Virulence Genes and Antibiotic Resistance Characteristics of Klebsiella pneumoniae Clinical Isolates in Middle and East China.Infect Drug Resist. 2025 Mar 13;18:1451-1464. doi: 10.2147/IDR.S502323. eCollection 2025. Infect Drug Resist. 2025. PMID: 40098716 Free PMC article.
-
Prevalence of multidrug-resistant bacteria in healthcare and community settings in West Africa: systematic review and meta-analysis.BMC Infect Dis. 2025 Feb 28;25(1):292. doi: 10.1186/s12879-025-10562-w. BMC Infect Dis. 2025. PMID: 40022011 Free PMC article.
-
Medical Device-Associated Biofilm Infections and Multidrug-Resistant Pathogens.Pathogens. 2024 May 8;13(5):393. doi: 10.3390/pathogens13050393. Pathogens. 2024. PMID: 38787246 Free PMC article. Review.
References
-
- CDC. Antibiotic use in the United States, 2023 update: progress and opportunities. 2023. https://www.cdc.gov/antibiotic-use/stewardship-report/current.html. Accessed 06 Oct 2023.
-
- CDC. Antibiotic resistance threats in the United States. 2019. https://www.cdc.gov/drugresistance/pdf/threats-report/2019-ar-threats-re.... Accessed 06 Oct 2023.
-
- World Health Organization. Antimicrobial resistance. 2021. https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance. Accessed 06 Oct 2023.
-
- Bono MJ, Leslie SW, Reygaert WC. Urinary tract infection. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022. https://www.ncbi.nlm.nih.gov/books/NBK470195/. Accessed 06 Oct 2023.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
