

Association between pregnancy-related complications and development of type 2 diabetes and hypertension in women: an umbrella review
- PMID: 38355631
- PMCID: PMC10865714
- DOI: 10.1186/s12916-024-03284-4
Association between pregnancy-related complications and development of type 2 diabetes and hypertension in women: an umbrella review
Abstract
Background: Despite many systematic reviews and meta-analyses examining the associations of pregnancy complications with risk of type 2 diabetes mellitus (T2DM) and hypertension, previous umbrella reviews have only examined a single pregnancy complication. Here we have synthesised evidence from systematic reviews and meta-analyses on the associations of a wide range of pregnancy-related complications with risk of developing T2DM and hypertension.
Methods: Medline, Embase and Cochrane Database of Systematic Reviews were searched from inception until 26 September 2022 for systematic reviews and meta-analysis examining the association between pregnancy complications and risk of T2DM and hypertension. Screening of articles, data extraction and quality appraisal (AMSTAR2) were conducted independently by two reviewers using Covidence software. Data were extracted for studies that examined the risk of T2DM and hypertension in pregnant women with the pregnancy complication compared to pregnant women without the pregnancy complication. Summary estimates of each review were presented using tables, forest plots and narrative synthesis and reported following Preferred Reporting Items for Overviews of Reviews (PRIOR) guidelines.
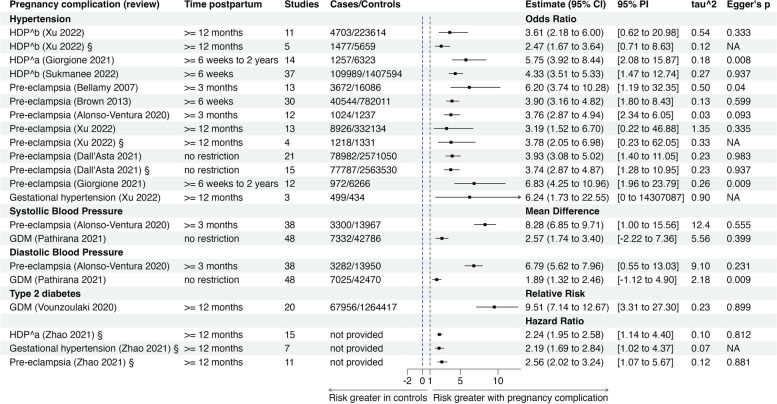
Results: Ten systematic reviews were included. Two pregnancy complications were identified. Gestational diabetes mellitus (GDM): One review showed GDM was associated with a 10-fold higher risk of T2DM at least 1 year after pregnancy (relative risk (RR) 9.51 (95% confidence interval (CI) 7.14 to 12.67) and although the association differed by ethnicity (white: RR 16.28 (95% CI 15.01 to 17.66), non-white: RR 10.38 (95% CI 4.61 to 23.39), mixed: RR 8.31 (95% CI 5.44 to 12.69)), the between subgroups difference were not statistically significant at 5% significance level. Another review showed GDM was associated with higher mean blood pressure at least 3 months postpartum (mean difference in systolic blood pressure: 2.57 (95% CI 1.74 to 3.40) mmHg and mean difference in diastolic blood pressure: 1.89 (95% CI 1.32 to 2.46) mmHg). Hypertensive disorders of pregnancy (HDP): Three reviews showed women with a history of HDP were 3 to 6 times more likely to develop hypertension at least 6 weeks after pregnancy compared to women without HDP (meta-analysis with largest number of studies: odds ratio (OR) 4.33 (3.51 to 5.33)) and one review reported a higher rate of T2DM after HDP (hazard ratio (HR) 2.24 (1.95 to 2.58)) at least a year after pregnancy. One of the three reviews and five other reviews reported women with a history of preeclampsia were 3 to 7 times more likely to develop hypertension at least 6 weeks postpartum (meta-analysis with the largest number of studies: OR 3.90 (3.16 to 4.82) with one of these reviews reporting the association was greatest in women from Asia (Asia: OR 7.54 (95% CI 2.49 to 22.81), Europe: OR 2.19 (95% CI 0.30 to 16.02), North and South America: OR 3.32 (95% CI 1.26 to 8.74)).
Conclusions: GDM and HDP are associated with a greater risk of developing T2DM and hypertension. Common confounders adjusted for across the included studies in the reviews were maternal age, body mass index (BMI), socioeconomic status, smoking status, pre-pregnancy and current BMI, parity, family history of T2DM or cardiovascular disease, ethnicity, and time of delivery. Further research is needed to evaluate the value of embedding these pregnancy complications as part of assessment for future risk of T2DM and chronic hypertension.
Keywords: Hypertension; Obstetrics and gynaecology; Pregnancy complications; Type 2 diabetes; Umbrella review.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Fraser A, Nelson SM, Macdonald-Wallis C, Cherry L, Butler E, Sattar N, et al. Associations of pregnancy complications with calculated cardiovascular disease risk and cardiovascular risk factors in middle age: the avon longitudinal study of parents and children. Circulation. 2012;125(11):1367–1380. doi: 10.1161/CIRCULATIONAHA.111.044784. - DOI - PMC - PubMed
-
- Bosio PM, McKenna PJ, Conroy R, O’Herlihy C. Maternal central hemodynamics in hypertensive disorders of pregnancy. Obstet Gynecol. 1999;94(6):978–984. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
