

Assessing respiratory epidemic potential in French hospitals through collection of close contact data (April-June 2020)
- PMID: 38355640
- PMCID: PMC10866902
- DOI: 10.1038/s41598-023-50228-8
Assessing respiratory epidemic potential in French hospitals through collection of close contact data (April-June 2020)
Abstract
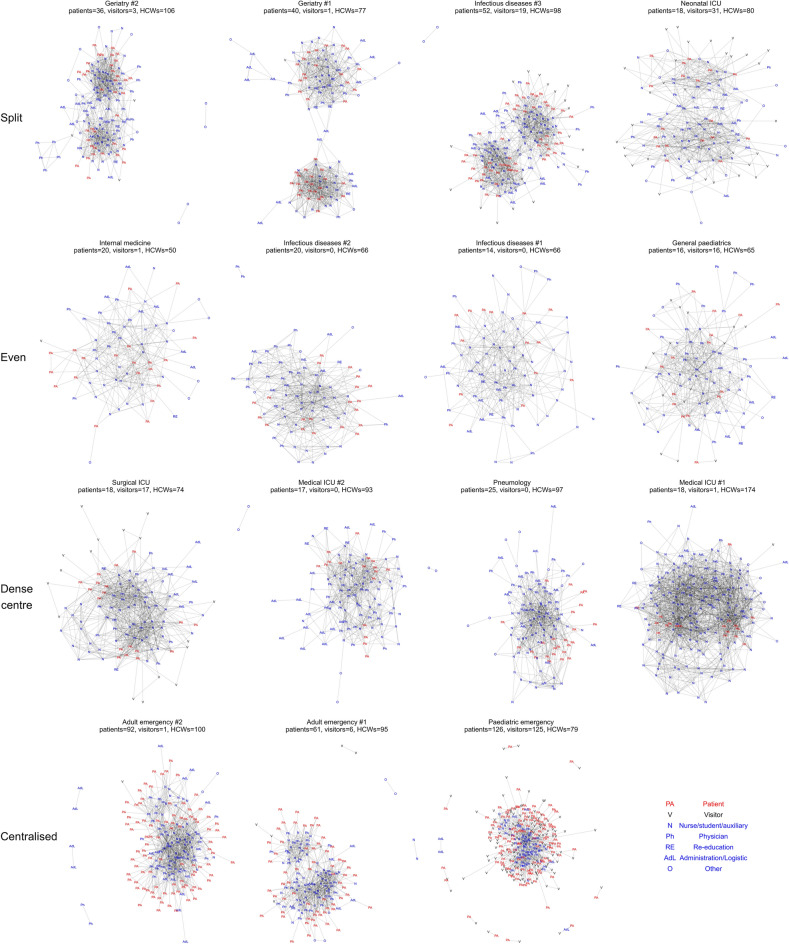
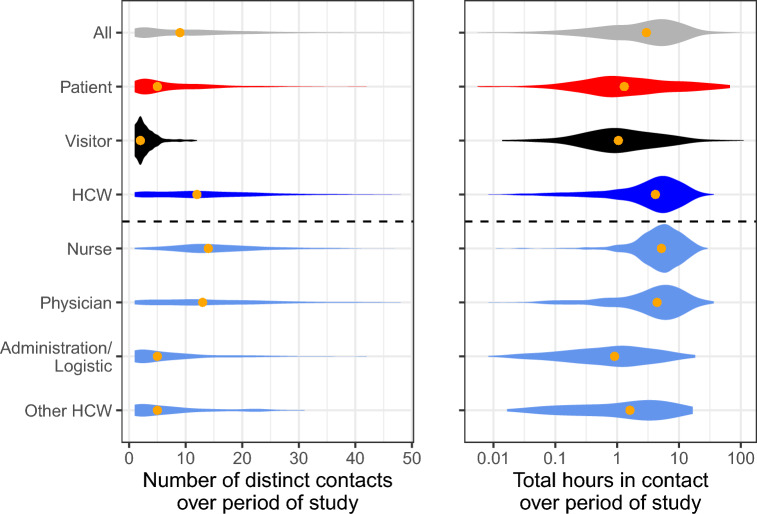
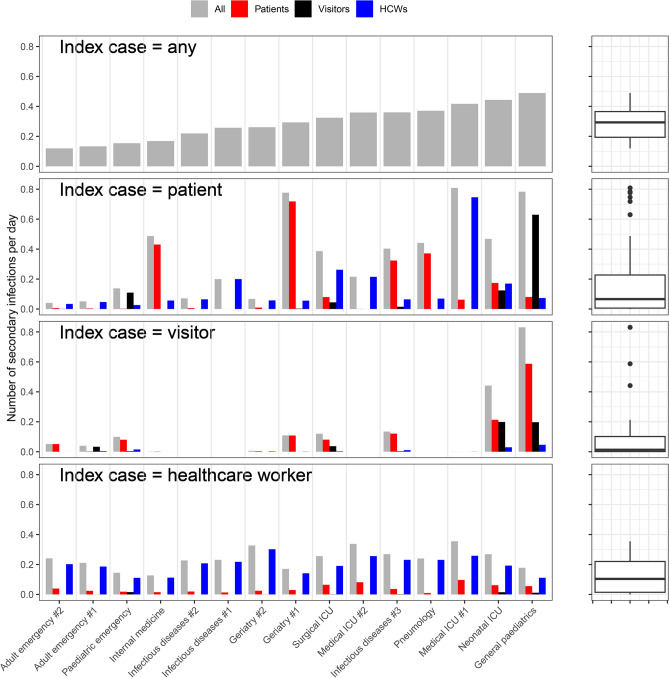
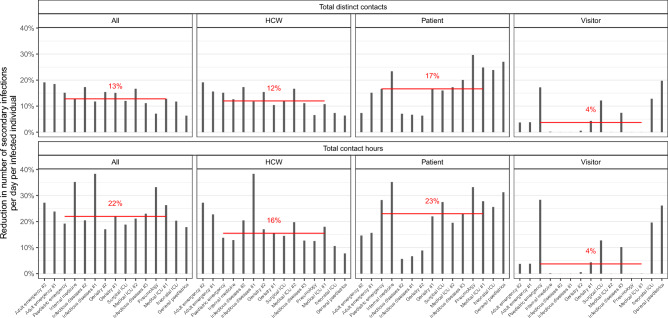
The transmission risk of SARS-CoV-2 within hospitals can exceed that in the general community because of more frequent close proximity interactions (CPIs). However, epidemic risk across wards is still poorly described. We measured CPIs directly using wearable sensors given to all present in a clinical ward over a 36-h period, across 15 wards in three hospitals in April-June 2020. Data were collected from 2114 participants and combined with a simple transmission model describing the arrival of a single index case to the ward to estimate the risk of an outbreak. Estimated epidemic risk ranged four-fold, from 0.12 secondary infections per day in an adult emergency to 0.49 per day in general paediatrics. The risk presented by an index case in a patient varied 20-fold across wards. Using simulation, we assessed the potential impact on outbreak risk of targeting the most connected individuals for prevention. We found that targeting those with the highest cumulative contact hours was most impactful (20% reduction for 5% of the population targeted), and on average resources were better spent targeting patients. This study reveals patterns of interactions between individuals in hospital during a pandemic and opens new routes for research into airborne nosocomial risk.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
