Active Surveillance for Low-Risk Thyroid Cancers: A Review of Current Practice Guidelines
- PMID: 38356210
- PMCID: PMC10901665
- DOI: 10.3803/EnM.2024.1937
Active Surveillance for Low-Risk Thyroid Cancers: A Review of Current Practice Guidelines
Abstract
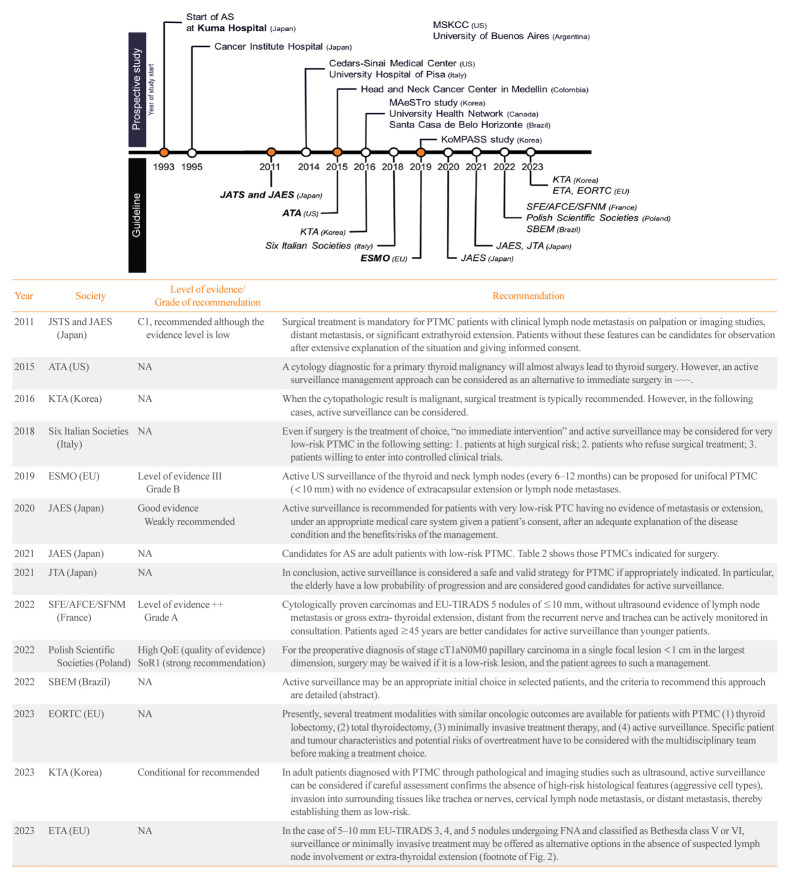
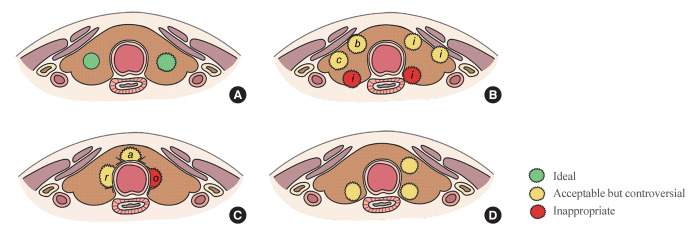
The indolent nature and favorable outcomes associated with papillary thyroid microcarcinoma have prompted numerous prospective studies on active surveillance (AS) and its adoption as an alternative to immediate surgery in managing low-risk thyroid cancer. This article reviews the current status of AS, as outlined in various international practice guidelines. AS is typically recommended for tumors that measure 1 cm or less in diameter and do not exhibit aggressive subtypes on cytology, extrathyroidal extension, lymph node metastasis, or distant metastasis. To determine the most appropriate candidates for AS, factors such as tumor size, location, multiplicity, and ultrasound findings are considered, along with patient characteristics like medical condition, age, and family history. Moreover, shared decision-making, which includes patient-reported outcomes such as quality of life and cost-effectiveness, is essential. During AS, patients undergo regular ultrasound examinations to monitor for signs of disease progression, including tumor growth, extrathyroidal extension, or lymph node metastasis. In conclusion, while AS is a feasible and reliable approach for managing lowrisk thyroid cancer, it requires careful patient selection, effective communication for shared decision-making, standardized follow-up protocols, and a clear definition of disease progression.
Keywords: Active surveillance; Guideline; Papillary thyroid cancer; Practice guideline; Thyroid neoplasms; Watchful waiting.
Conflict of interest statement
Young Joo Park is an editor-in-chief of the journal. But she was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflicts of interest relevant to this article were reported.
Figures
Similar articles
-
Standardized Ultrasound Evaluation for Active Surveillance of Low-Risk Thyroid Microcarcinoma in Adults: 2024 Korean Society of Thyroid Radiology Consensus Statement.Korean J Radiol. 2024 Nov;25(11):942-958. doi: 10.3348/kjr.2024.0871. Korean J Radiol. 2024. PMID: 39473087 Free PMC article.
-
Progression of Low-Risk Papillary Thyroid Microcarcinoma During Active Surveillance: Interim Analysis of a Multicenter Prospective Cohort Study of Active Surveillance on Papillary Thyroid Microcarcinoma in Korea.Thyroid. 2022 Nov;32(11):1328-1336. doi: 10.1089/thy.2021.0614. Thyroid. 2022. PMID: 36205563 Free PMC article.
-
Ultrasound Imaging Criteria and Protocols for Active Surveillance of Low-Risk Thyroid Cancer: A Review of International Consensus Guidelines.Endocrinol Metab (Seoul). 2025 Apr;40(2):185-194. doi: 10.3803/EnM.2024.2319. Epub 2025 Mar 27. Endocrinol Metab (Seoul). 2025. PMID: 40140733 Free PMC article. Review.
-
Standardized Ultrasound Evaluation for Active Surveillance of Low-Risk Thyroid Microcarcinoma in Adults: 2024 Korean Society of Thyroid Radiology Consensus Statement.J Korean Soc Radiol. 2024 Nov;85(6):1060-1082. doi: 10.3348/jksr.2024.0132. Epub 2024 Nov 15. J Korean Soc Radiol. 2024. PMID: 39660311 Free PMC article. Review.
-
Active surveillance of low-risk papillary thyroid microcarcinoma.Best Pract Res Clin Endocrinol Metab. 2023 Jan;37(1):101630. doi: 10.1016/j.beem.2022.101630. Epub 2022 Feb 24. Best Pract Res Clin Endocrinol Metab. 2023. PMID: 35256266 Review.
Cited by
-
Advances in clinical research on ultrasound-guided radiofrequency ablation for papillary thyroid microcarcinoma.Front Oncol. 2024 Jul 8;14:1422634. doi: 10.3389/fonc.2024.1422634. eCollection 2024. Front Oncol. 2024. PMID: 39040438 Free PMC article.
-
Assessing the Rise in Papillary Thyroid Cancer Incidence: A 38-Year Australian Study Investigating WHO Classification Influence.J Epidemiol Glob Health. 2025 Jan 27;15(1):9. doi: 10.1007/s44197-025-00354-5. J Epidemiol Glob Health. 2025. PMID: 39869269 Free PMC article.
-
Proteomic Analysis of Tissue Proteins Related to Lateral Lymph Node Metastasis in Papillary Thyroid Microcarcinoma.J Proteome Res. 2025 Jan 3;24(1):256-267. doi: 10.1021/acs.jproteome.4c00737. Epub 2024 Nov 27. J Proteome Res. 2025. PMID: 39600146 Free PMC article.
-
Study Protocol of Expanded Multicenter Prospective Cohort Study of Active Surveillance on Papillary Thyroid Microcarcinoma (MAeSTro-EXP) (Endocrinol Metab 2025;40:236-46, Jae Hoon Moon et al.).Endocrinol Metab (Seoul). 2025 Aug;40(4):655-656. doi: 10.3803/EnM.2025.2495. Epub 2025 Jul 23. Endocrinol Metab (Seoul). 2025. PMID: 40701182 Free PMC article. No abstract available.
-
A national survey of physicians regarding active surveillance for low-risk thyroid cancer in Korea.Eur Thyroid J. 2025 Jan 9;14(1):e240281. doi: 10.1530/ETJ-24-0281. Print 2025 Feb 1. Eur Thyroid J. 2025. PMID: 39656545 Free PMC article.
References
-
- Pizzato M, Li M, Vignat J, Laversanne M, Singh D, La Vecchia C, et al. The epidemiological landscape of thyroid cancer worldwide: GLOBOCAN estimates for incidence and mortality rates in 2020. Lancet Diabetes Endocrinol. 2022;10:264–72. - PubMed
-
- Vaccarella S, Franceschi S, Bray F, Wild CP, Plummer M, Dal Maso L. Worldwide thyroid-cancer epidemic?: the increasing impact of overdiagnosis. N Engl J Med. 2016;375:614–7. - PubMed
-
- Ahn HS, Kim HJ, Welch HG. Korea’s thyroid-cancer “epidemic”: screening and overdiagnosis. N Engl J Med. 2014;371:1765–7. - PubMed
-
- Harach HR, Franssila KO, Wasenius VM. Occult papillary carcinoma of the thyroid: a “normal” finding in Finland: a systematic autopsy study. Cancer. 1985;56:531–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials