

Editorial
doi: 10.3324/haematol.2023.284534.
Indirect treatment comparisons: how to MAIC it right?
Affiliations
- PMID: 38356445
- PMCID: PMC11215367
- DOI: 10.3324/haematol.2023.284534
Item in Clipboard
Editorial
Indirect treatment comparisons: how to MAIC it right?
Haematologica.
.
No abstract available
Figures
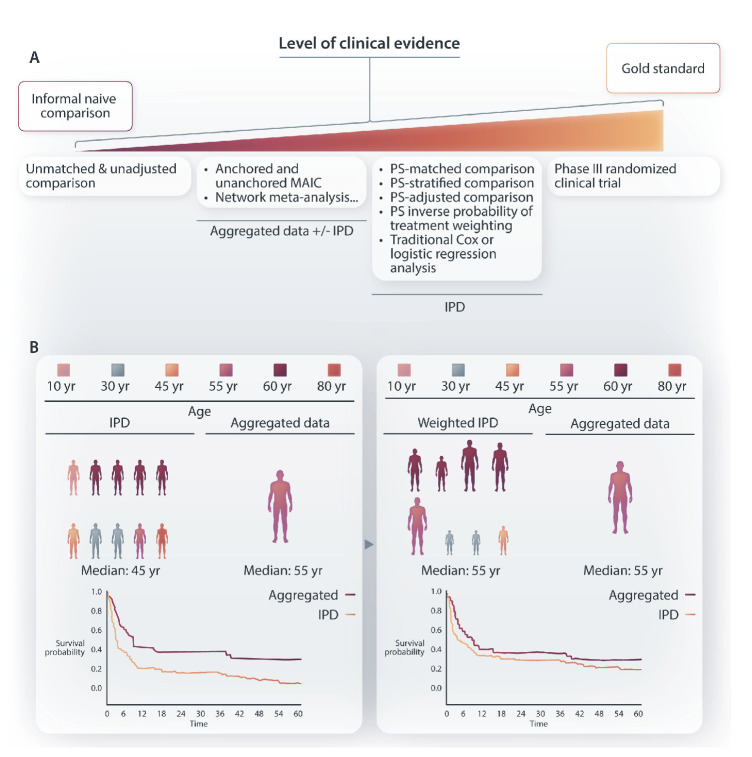
Principle and level of clinical evidence of matching-adjusted indirect comparison. (A) Level of evidence of various treatment comparisons from unadjusted and unmatched comparison (poorest level of evidence) to randomized treatment allocation (gold standard). The list of various statistical approaches to make patient population as comparable as possible is not exhaustive. (B) Matching-adjusted indirect comparison (MAIC) allows for the comparison between aggregated patient data (e.g., based on patient characteristics from a trial publication) and individual patient data (from another trial or a real-life cohort or any other source of individual data). Basically, by removing or pondering patient characteristics to closely match final aggregated data (e.g., patient median age depicted here), the final group of patients from the cohort with available individual patient data (IPD) is rendered as similar as possible to the cohort for which only aggregated data are available (e.g., here, similar median age). This is performed for all variables that are considered as critical confounders for treatment comparison. Finally, outcome is compared in the 2 matched populations; here, the prognosis of the IPD is depicted as better after matching (blue line), while, by definition, the survival of the aggregated data population is left unchanged after matching (red line). Depicted data and survivals are for illustration only and are not based on true or relevant values or weights. PS: propensity score; yr: year.
Similar articles
-
Evaluation of Adjusted and Unadjusted Indirect Comparison Methods in Benefit Assessment. A Simulation Study for Time-to-event Endpoints.Methods Inf Med. 2017 May 18;56(3):261-267. doi: 10.3414/ME15-02-0016. Epub 2017 Mar 31. Methods Inf Med. 2017. PMID: 28361159
-
On the double-robustness and semiparametric efficiency of matching-adjusted indirect comparisons.Res Synth Methods. 2023 May;14(3):438-442. doi: 10.1002/jrsm.1616. Epub 2023 Jan 3. Res Synth Methods. 2023. PMID: 36537355
-
Matching-adjusted indirect comparison (MAIC) results confirmed by head-to-head trials: a case study in psoriasis.J Dermatolog Treat. 2023 Dec;34(1):2169574. doi: 10.1080/09546634.2023.2169574. J Dermatolog Treat. 2023. PMID: 36724798
-
Methods for population adjustment with limited access to individual patient data: A review and simulation study.Res Synth Methods. 2021 Nov;12(6):750-775. doi: 10.1002/jrsm.1511. Epub 2021 Sep 5. Res Synth Methods. 2021. PMID: 34196111 Review.
-
Comparative Efficacy and Safety of Ozanimod and Dimethyl Fumarate for Relapsing-Remitting Multiple Sclerosis Using Matching-Adjusted Indirect Comparison.CNS Drugs. 2021 Jul;35(7):795-804. doi: 10.1007/s40263-021-00805-0. Epub 2021 Apr 13. CNS Drugs. 2021. PMID: 33847901 Free PMC article.
References
-
- Maurer MJ, Casulo C, Larson MC, et al. . Matching-adjusted indirect comparison from the Lymphoma Epidemiology of Outcomes Consortium for Real World Evidence (LEO CReWE) study to a clinical trial of mosunetuzumab in relapsed or refractory follicular lymphoma. Haematologica. 2024;109(7):2177-2185. - PMC - PubMed
-
- Budde LE, Sehn LH, Matasar M, et al. . Safety and efficacy of mosunetuzumab, a bispecific antibody, in patients with relapsed or refractory follicular lymphoma: a single-arm, multicentre, phase 2 study. Lancet Oncol. 2022;23(8):1055-1065. - PubMed
-
- Signorovitch JE, Wu EQ, Yu AP, et al. . Comparative effectiveness without head-to-head trials: a method for matching-adjusted indirect comparisons applied to psoriasis treatment with adalimumab or etanercept. Pharmacoeconomics. 2010;28(10):935-945. - PubMed
-
- Signorovitch JE, Sikirica V, Erder MH, et al. . Matching-adjusted indirect comparisons: a new tool for timely comparative effectiveness research. Value Health. 2012;15(6):940-947. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
