

Combining Charlson comorbidity and VACS indices improves prognostic accuracy for all-cause mortality for patients with and without HIV in the Veterans Health Administration
- PMID: 38356736
- PMCID: PMC10864663
- DOI: 10.3389/fmed.2023.1342466
Combining Charlson comorbidity and VACS indices improves prognostic accuracy for all-cause mortality for patients with and without HIV in the Veterans Health Administration
Erratum in
-
Corrigendum: Combining Charlson comorbidity and VACS indices improves prognostic accuracy for all-cause mortality for patients with and without HIV in the Veterans Health Administration.Front Med (Lausanne). 2025 Jan 8;11:1532350. doi: 10.3389/fmed.2024.1532350. eCollection 2024. Front Med (Lausanne). 2025. PMID: 39845833 Free PMC article.
Abstract
Introduction: As people age with HIV (PWH), many comorbid diseases are more common than among age matched comparators without HIV (PWoH). While the Veterans Aging Cohort (VACS) Index 2.0 accurately predicts mortality in PWH using age and clinical biomarkers, the only included comorbidity is hepatitis C. We asked whether adding comorbid disease groupings from the Charlson Comorbidity Index (CCI) improves the accuracy of VACS Index.
Methods: To maximize our ability to model mortality among older age groups, we began with PWoH in Veterans Health Administration (VA) from 2007-2017, divided into development and validation samples. Baseline predictors included age, and components of CCI and VACS Index (excluding CD4 count and HIV RNA). Patients were followed until December 31, 2021. We used Cox models to develop the VACS-CCI score and estimated mortality using a parametric (gamma) survival model. We compared accuracy using C-statistics and calibration curves in validation overall and within subgroups (gender, age </≥65 years, race/ethnicity, and CCI score). We then applied VACS-CCI in PWH and compared its accuracy to age, VACS Index 2.0, CCI and VACS-CCI with CD4 and HIV RNA added.
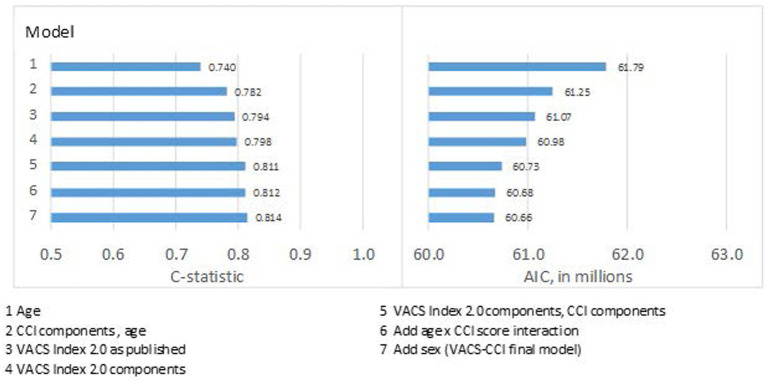
Results: The analytic sample consisted of 6,588,688 PWoH and 30,539 PWH. Among PWoH/PWH, median age was 65/55 years; 6%/3% were women; 15%/48% were Black and 5%/7% Hispanic. VACS-CCI provided the best discrimination (C-statistic = 0.81) with excellent calibration (predicted and observed mortality largely overlapped) overall and within subgroups. When VACS-CCI was applied to PWH it demonstrated similar discrimination as VACS Index 2.0 (C-statistic = 0.77 for both) but superior calibration among those with CD4 < 200. Discrimination was improved when CD4 and HIV RNA were added VACS-CCI (C-statistic = 0.79). Liver and kidney disease, congestive heart failure, malignancy, and dementia were negatively associated with CD4 (p-trends all <0.0001).
Discussion: Among PWH and PWoH in VA care, age alone weakly discriminates risk of mortality. VACS Index 2.0, CCI, and VACS-CCI all provide better discrimination, but VACS-CCI is more consistently calibrated. The association of comorbid diseases with lower CD4 underscores the likely role of HIV in non-AIDS conditions. Future work will include adding CD4 and HIV RNA to VACS-CCI and validating it in independent data.
Keywords: Charlson Comorbidity Index; HIV; VACS Index; mortality; prediction.
Copyright © 2024 McGinnis, Justice, Marconi, Rodriguez-Barradas, Hauser, Oursler, Brown, Bryant and Tate.
Conflict of interest statement
VM has received investigator-initiated research grants (to the institution) and consultation fees from Eli Lilly, Bayer, Gilead Sciences, Merck, and ViiV. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures




References
-
- Althoff KN, McGinnis KA, Wyatt CM, Freiberg MS, Gilbert C, Oursler KK, et al. Comparison of risk and age at diagnosis of myocardial infarction, end-stage renal disease, and non-AIDS-defining cancer in HIV-infected versus uninfected adults. Clin Infect Dis. (2015) 60:627–38. doi: 10.1093/cid/ciu869, PMID: - DOI - PMC - PubMed
-
- Hogg RS, Eyawo O, Collins AB, Zhang W, Jabbari S, Hull MW, et al. Health-adjusted life expectancy in HIV-positive and HIV-negative men and women in British Columbia, Canada: a population-based observational cohort study. The measurement of health adjusted life expectancy (HALE) on a population-based observational cohort of HIV-positive and negative men and women in British Columbia. Lancet HIV. (2017) 4:e270–6. doi: 10.1016/S2352-3018(17)30029-2 - DOI - PMC - PubMed
-
- Park LS, Tate JP, Sigel K, Brown ST, Crothers K, Gibert C, et al. Association of Viral Suppression with Lower AIDS-defining and non-AIDS-defining Cancer incidence in HIV-infected veterans: a prospective cohort study. Ann Intern Med. (2018) 169:87–96. doi: 10.7326/M16-2094, PMID: - DOI - PMC - PubMed
-
- Althoff KN, Chandran A, Zhang J, Arevalo WM, Gange SJ, Sterling TR, et al. Life-expectancy disparities among adults with HIV in the United States and Canada: the impact of a reduction in drug- and alcohol-related deaths using the lives saved simulation model. Am J Epidemiol. (2019) 188:2097–109. doi: 10.1093/aje/kwz232, PMID: - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials