

Accurate diagnosis and treatment of sacral meningeal cysts without spinal nerve root fibres: identifying leakage orificium using high-resolution spherical arbitrary-dimensional reconstructing magnetic resonance imaging
- PMID: 38356887
- PMCID: PMC10865724
- DOI: 10.3389/fneur.2024.1298477
Accurate diagnosis and treatment of sacral meningeal cysts without spinal nerve root fibres: identifying leakage orificium using high-resolution spherical arbitrary-dimensional reconstructing magnetic resonance imaging
Abstract
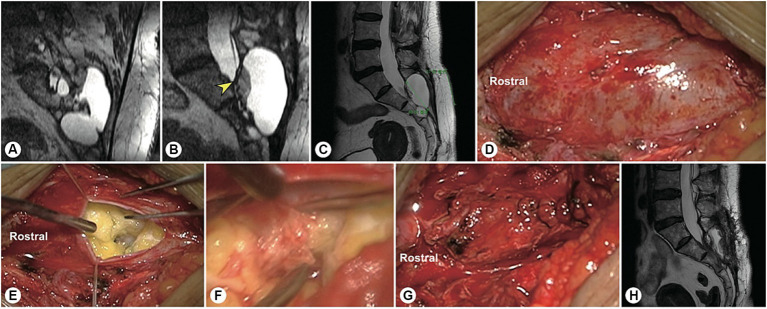
Objective: This study aimed to develop an arbitrary-dimensional nerve root reconstruction magnetic resonance imaging (ANRR-MRI) technique for identifying the leakage orificium of sacral meningeal cysts (SMCs) without spinal nerve root fibres (SNRFs).
Methods: This prospective study enrolled 40 consecutive patients with SMCs without SNRFs between March 2021 and March 2022. Magnetic resonance neural reconstruction sequences were performed for preoperative evaluation. The cyst and the cyst-dura intersection planes were initially identified based on the original thin-slice axial T2-weighted images. Sagittal and coronal images were then reconstructed by setting each intersecting plane as the centre. Then, three-dimensional reconstruction was performed, focusing on the suspected leakage point of the cyst. Based on the identified leakage location and size of the SMC, individual surgical plans were formulated.
Results: This cohort included 30 females and 10 males, with an average age of 42.6 ± 12.2 years (range, 17-66 years). The leakage orificium was located at the rostral pole of the cyst in 23 patients, at the body region of the cyst in 12 patients, and at the caudal pole in 5 patients. The maximum diameter of the cysts ranged from 2 cm to 11 cm (average, 5.2 ± 1.9 cm). The leakage orificium was clearly identified in all patients and was ligated microscopically through a 4 cm minimally invasive incision. Postoperative imaging showed that the cysts had disappeared.
Conclusion: ANRR-MRI is an accurate and efficient approach for identifying leakage orificium, facilitating the precise diagnosis and surgical treatment of SMCs without SNRFs.
Keywords: leakage orificium; magnetic resonance imaging; sacral cyst; sectional reconstruction; spinal nerve root.
Copyright © 2024 Yang, Lou, Huang, Ma, Yin, Zhao, Wu, Wu and Sun.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The reviewer HT declared a shared affiliation with the author JS to the handling editor at the time of review.
Figures






Similar articles
-
[Significance of precise classification of sacral meningeal cysts by multiple dimensions radiographic reconstruction MRI in guiding operative strategy and rehabilitation].Beijing Da Xue Xue Bao Yi Xue Ban. 2025 Apr 18;57(2):303-308. doi: 10.19723/j.issn.1671-167X.2025.02.013. Beijing Da Xue Xue Bao Yi Xue Ban. 2025. PMID: 40219561 Free PMC article. Chinese.
-
Multiple dimensions of radiographic reconstruction for the optimal operative strategy of sacral meningeal cysts.Eur Spine J. 2022 Nov;31(11):3146-3158. doi: 10.1007/s00586-022-07337-1. Epub 2022 Aug 10. Eur Spine J. 2022. PMID: 35947195
-
Persistent Genital Arousal Disorder Caused by Spinal Meningeal Cysts in the Sacrum: Successful Neurosurgical Treatment.Obstet Gynecol. 2015 Oct;126(4):839-843. doi: 10.1097/AOG.0000000000001060. Obstet Gynecol. 2015. PMID: 26348167
-
[Spinal cysts : Diagnostic workup and therapy].Radiologe. 2018 Feb;58(2):113-119. doi: 10.1007/s00117-017-0350-8. Radiologe. 2018. PMID: 29411052 Review. German.
-
Symptomatic spinal intradural arachnoid cysts in the pediatric age group: description of three new cases and review of the literature.Pediatr Neurosurg. 2001 Oct;35(4):181-7. doi: 10.1159/000050419. Pediatr Neurosurg. 2001. PMID: 11694795 Review.
Cited by
-
Editorial: Integrated clinical management and neurorehabilitation for lumbosacral spinal diseases.Front Neurol. 2025 Jun 24;16:1590602. doi: 10.3389/fneur.2025.1590602. eCollection 2025. Front Neurol. 2025. PMID: 40630910 Free PMC article. No abstract available.
References
LinkOut - more resources
Full Text Sources