

A systematic-search-and-review of registered pharmacological therapies investigated to improve neuro-recovery after a stroke
- PMID: 38356890
- PMCID: PMC10866005
- DOI: 10.3389/fneur.2024.1346177
A systematic-search-and-review of registered pharmacological therapies investigated to improve neuro-recovery after a stroke
Abstract
Background: Stroke burden is largely due to long-term impairments requiring prolonged care with loss of productivity. We aimed to identify and assess studies of different registered pharmacological therapies as treatments to improve post-stroke impairments and/or disabilities.
Methods: We performed a systematic-search-and-review of treatments that have been investigated as recovery-enhancing or recovery-promoting therapies in adult patients with stroke. The treatment must have received registration or market authorization in any country regardless of primary indication. Outcomes included in the review were neurological impairments and functional/disability assessments. "The best available studies" based on study design, study size, and/or date of publication were selected and graded for level of evidence (LOE) by consensus.
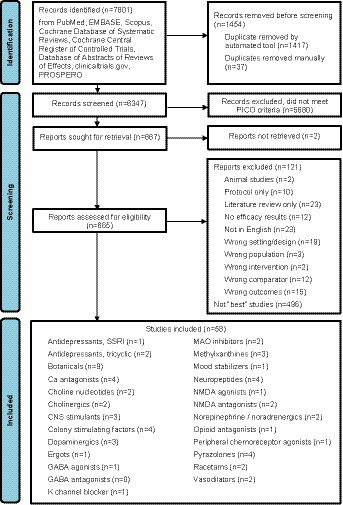
Results: Our systematic search yielded 7,801 citations, and we reviewed 665 full-text papers. Fifty-eight publications were selected as "the best studies" across 25 pharmacological classes: 31 on ischemic stroke, 21 on ischemic or hemorrhagic stroke, 4 on intracerebral hemorrhage, and 2 on subarachnoid hemorrhage (SAH). Twenty-six were systematic reviews/meta-analyses, 29 were randomized clinical trials (RCTs), and three were cohort studies. Only nimodipine for SAH had LOE A of benefit (systematic review and network meta-analysis). Many studies, some of which showed treatment effects, were assessed as LOE C-LD, mainly due to small sample sizes or poor quality. Seven interventions had LOE B-R (systematic review/meta-analysis or RCT) of treatment effects.
Conclusion: Only one commercially available treatment has LOE A for routine use in stroke. Further studies of putative neuroprotective drugs as adjunctive treatment to revascularization procedures and more confirmatory trials on recovery-promoting therapies will enhance the certainty of their benefit. The decision on their use must be guided by the clinical profile, neurological impairments, and target outcomes based on the available evidence.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=376973, PROSPERO, CRD42022376973.
Keywords: evidence; neuro-restoration; recovery; rehabilitation; review; stroke.
Copyright © 2024 Lee, Uchiyama, Kusuma, Chiu, Navarro, Tan, Pandian, Guo, Wong and Venketasubramanian.
Conflict of interest statement
SU received funding for clinical trials related to edaravone, but was not involved in the assessment of edaravone for this paper. JCN received funding for clinical trials related to MLC601/MLC901. He was not involved in the assessment of MLC601/MLC901 for this paper. NV received funding for clinical trials related to MLC601/MLC901 that were paid to his institution. He was not involved in the assessment of MLC601/MLC901 for this paper. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
References
-
- Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. . Guidelines for the early Management of Patients with acute ischemic Stroke: 2019 update to the 2018 guidelines for the early Management of Acute Ischemic Stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2019) 50:e344–418. doi: 10.1161/STR.0000000000000211 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials