

Does perinatal management have the potential to reduce the risk of intraventricular hemorrhage in preterm infants?
- PMID: 38357510
- PMCID: PMC10864433
- DOI: 10.3389/fped.2024.1361074
Does perinatal management have the potential to reduce the risk of intraventricular hemorrhage in preterm infants?
Abstract
Background: Intraventricular hemorrhage (IVH) is an important cause of neurodevelopmental impairment in preterm infants. A number of risk factors for IVH have already been proposed; however, some controversies regarding optimal perinatal management persist. This study aimed to identify perinatal and neonatal attributes associated with IVH in a representative population of preterm infants.
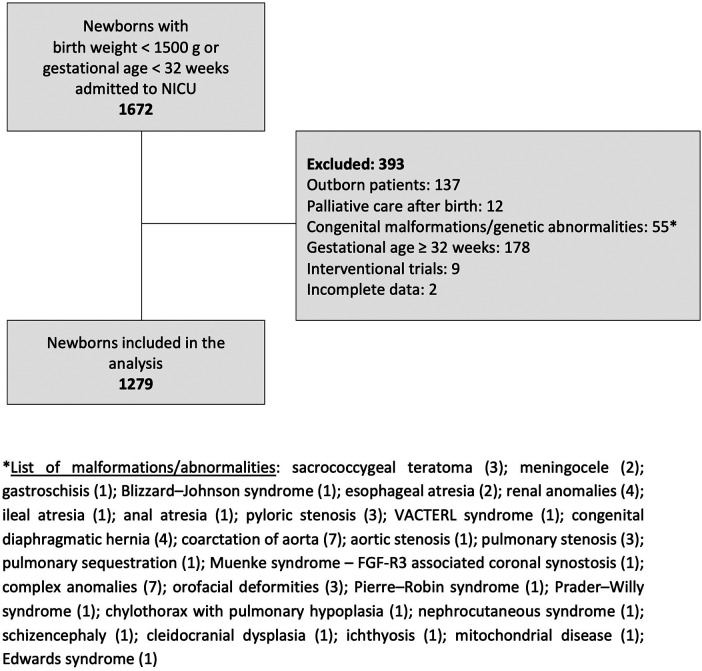
Methods: Perinatal data on 1,279 very preterm infants (<32 weeks of gestation) admitted to a tertiary neonatal intensive care unit were analyzed. The records were assessed using univariate analysis and logistic regression model to evaluate the risk factors for any and high-grade IVH (grade III-IV according to the classification by Papile) within the first week after birth.
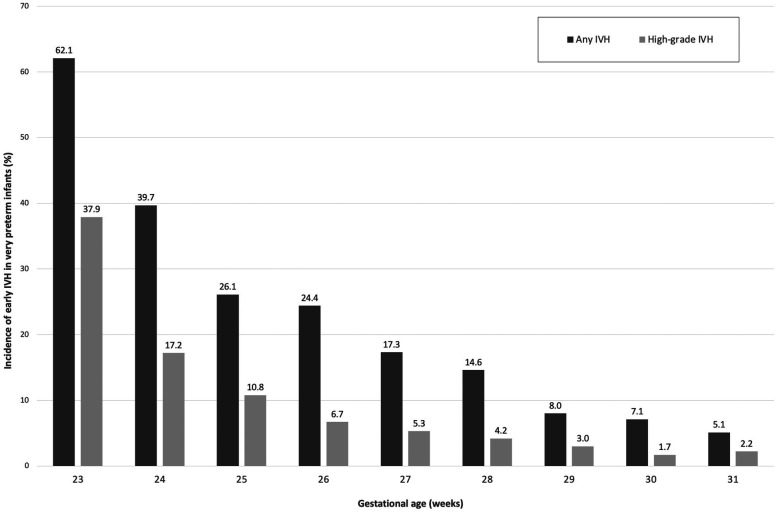
Results: The incidence of any IVH was 14.3% (183/1,279); the rate of low-grade (I-II) and high-grade (III-IV) IVH was 9.0% (115/1,279) and 5.3% (68/1,279), respectively. Univariate analysis revealed multiple factors significantly associated with intraventricular hemorrhage: lower gestational age and birth weight, absence of antenatal steroids, vaginal delivery, low Apgar score at 5 min, delivery room intubation, surfactant administration, high frequency oscillation, pulmonary hypertension, pulmonary hemorrhage, tension pneumothorax, persistent ductus arteriosus, hypotension and early onset sepsis. Logistic regression confirmed lower gestational age, vaginal delivery, ductus arteriosus and early onset sepsis to be independent predictors for any IVH. Pulmonary hemorrhage, tension pneumothorax and early onset sepsis were independent risk factors for high-grade IVH. Complete course of antenatal steroids was associated with a lower risk for any (odds ratio 0.58, 95% confidence interval 0.39-0.85; P = .006) and for high-grade intraventricular hemorrhage (odds ratio 0.36, 95% confidence interval 0.20-0.65; P < .001).
Conclusion: The use of antenatal steroids and mode of delivery are crucial in the prevention of IVH; however, our study did not confirm the protective effect of placental transfusion. Severe respiratory insufficiency and circulatory instability remain to be powerful contributors to the development of IVH. Early detection and management of perinatal infection may also help to reduce the rate of brain injury and improve neurodevelopment in high-risk newborns.
Keywords: antenatal steroids; early onset sepsis; intraventricular hemorrhage; mode of delivery; neonatal morbidity; perinatal management; preterm infants.
© 2024 Korček, Širc, Berka, Kučera and Straňák.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources