

No-reflow after stroke reperfusion therapy: An emerging phenomenon to be explored
- PMID: 38358074
- PMCID: PMC10867879
- DOI: 10.1111/cns.14631
No-reflow after stroke reperfusion therapy: An emerging phenomenon to be explored
Abstract
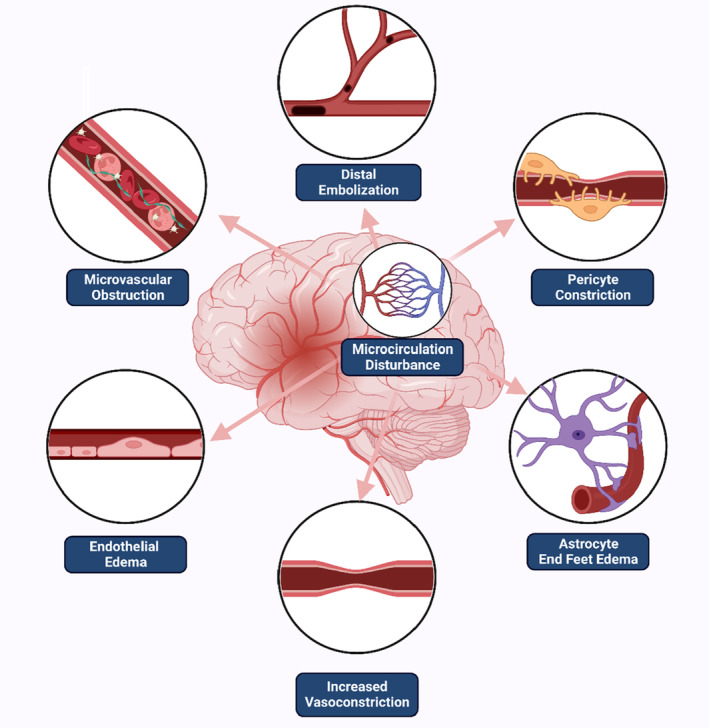
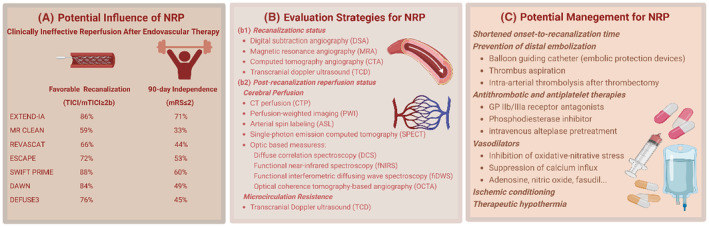
In the field of stroke thrombectomy, ineffective clinical and angiographic reperfusion after successful recanalization has drawn attention. Partial or complete microcirculatory reperfusion failure after the achievement of full patency of a former obstructed large vessel, known as the "no-reflow phenomenon" or "microvascular obstruction," was first reported in the 1960s and was later detected in both experimental models and patients with stroke. The no-reflow phenomenon (NRP) was reported to result from intraluminal occlusions formed by blood components and extraluminal constriction exerted by the surrounding structures of the vessel wall. More recently, an emerging number of clinical studies have estimated the prevalence of the NRP in stroke patients following reperfusion therapy, ranging from 3.3% to 63% depending on its evaluation methods or study population. Studies also demonstrated its detrimental effects on infarction progress and neurological outcomes. In this review, we discuss the research advances, underlying pathogenesis, diagnostic techniques, and management approaches concerning the no-reflow phenomenon in the stroke population to provide a comprehensive understanding of this phenomenon and offer references for future investigations.
Keywords: acute ischemic stroke; endovascular thrombectomy; microvascular disturbance; no-reflow phenomenon; reperfusion therapy.
© 2024 The Authors. CNS Neuroscience & Therapeutics published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Campbell BCV, Khatri P. Stroke. Lancet. 2020;396(10244):129‐142. - PubMed
-
- Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early Management of Patients with Acute Ischemic Stroke: 2019 update to the 2018 guidelines for the early Management of Acute Ischemic Stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344‐e418. - PubMed
-
- Rubiera M, Garcia‐Tornel A, Olivé‐Gadea M, et al. Computed tomography perfusion after thrombectomy: an immediate surrogate marker of outcome after recanalization in acute stroke. Stroke. 2020;51(6):1736‐1742. - PubMed
-
- Ng FC, Churilov L, Yassi N, et al. Prevalence and significance of impaired microvascular tissue reperfusion despite macrovascular angiographic reperfusion (No‐reflow). Neurology. 2022;98(8):e790‐e801. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
