

Frailty, periinterventional complications and outcome in patients undergoing percutaneous mitral and tricuspid valve repair
- PMID: 38358418
- PMCID: PMC12202524
- DOI: 10.1007/s00392-024-02397-3
Frailty, periinterventional complications and outcome in patients undergoing percutaneous mitral and tricuspid valve repair
Abstract
Background: Frailty is common in elderly and multimorbid patients and associated with increased vulnerability to stressors.
Methods: In a single centre study frailty according to Fried criteria was assessed in consecutive patients before transcatheter mitral and tricuspid valve repair. Postprocedural infections, blood transfusion and bleeding and renal failure were retrospectively assessed from records. Median follow-up time for survival was 560 days (IQR: 363 to 730 days).
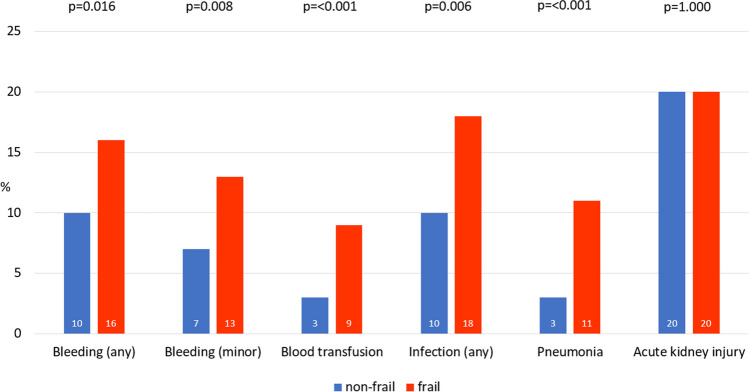
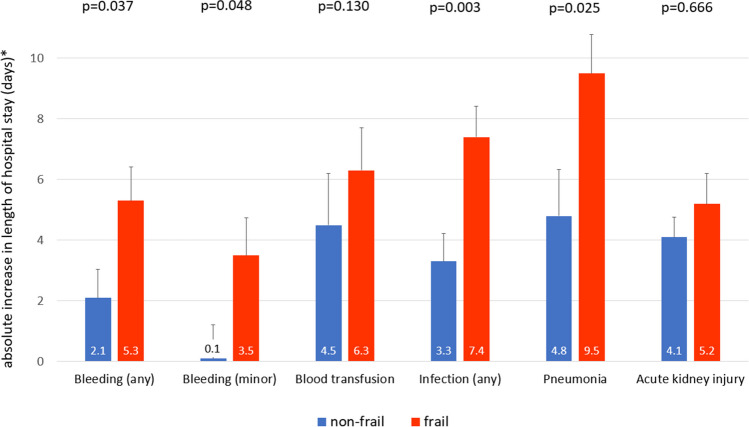
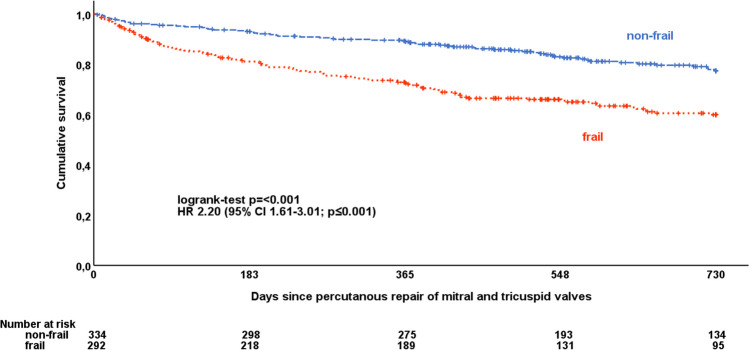
Results: 90% of 626 patients underwent mitral valve repair, 5% tricuspid valve repair, and 5% simultaneous mitral and tricuspid valve repair. 47% were classified as frail. Frailty was associated with a significantly increased frequency of bleeding (16 vs 10%; p = 0.016), blood transfusions (9 vs 3%; p = < 0.001) and infections (18 vs 10%; p = 0.006), but not with acute kidney injury (20 vs 20%; p = 1.00). Bleeding and infections were associated with longer hospital stays, with a more pronounced effect in frail patients (interaction test p < 0.05, additional 3.2 and 4.1 days in frail patients, respectively). Adjustment for the occurrence of complications did not attenuate the increased risk of mortality associated with frailty (HR 2.24 [95% CI 1.62-3.10]; p < 0.001).
Conclusions: Bleeding complications and infections were more frequent in frail patients undergoing transcatheter mitral and tricuspid valve repair and partly explained the longer hospital stay. Albeit some of the complications were associated with higher long-term mortality, this did not explain the strong association between frailty and mortality. Further research is warranted to explore interventions targeting periprocedural complications to improve outcomes in this vulnerable population.
Keywords: Acute Kidney Injury; Bleeding; Frailty; Infection; MitraClip.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: This study was performed in line with the principles of the Declaration of Helsinki. All enrolled patients gave written informed consent. The study was approved by the local ethics committee of the University of Cologne (14–116). Competing interests: CI has received travel support by Abbott Cardiovascular (Abbott Park, Chicago, US) and Edwards Lifesciences (Unterschleißheim, Germany) and consultant honoraria by Abbott and Edwards Lifesciences. MIC received travel support and proctor and lecture fees from Edwards lifesciences, Abbott and JenaValve (Irvine, US). RP received fees for presentations and consultancy by Edwards Lifesciences. SB received research grants and speaker honoraria by Edwards Lifesciences and Abbott and speaker honoraria from Medtronic (Dublin, Ireland). The other authors have no relevant financial or non-financial interests to disclose.
Figures
References
-
- Vahanian A, Beyersdorf F, Praz F et al (2022) 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J 43(7):561–632. 10.1093/eurheartj/ehab395 - PubMed
-
- Strandberg TE, Pitkälä KH (2007) Frailty in elderly people. Lancet 369(9570):1328–1329. 10.1016/s0140-6736(07)60613-8 - PubMed
-
- Malik AH, Yandrapalli S, Zaid S et al (2020) Impact of frailty on mortality, readmissions, and resource utilization after TAVI. Am J Cardiol 127:120–127. 10.1016/j.amjcard.2020.03.047 - PubMed
-
- Metze C, Matzik AS, Scherner M et al (2017) Impact of frailty on outcomes in patients undergoing percutaneous mitral valve repair. J Am Coll Cardiol Intv 10(19):1920–1929. 10.1016/j.jcin.2017.07.042 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
