

Routes of Drug Use Among Drug Overdose Deaths - United States, 2020-2022
- PMID: 38358969
- PMCID: PMC10899081
- DOI: 10.15585/mmwr.mm7306a2
Routes of Drug Use Among Drug Overdose Deaths - United States, 2020-2022
Abstract
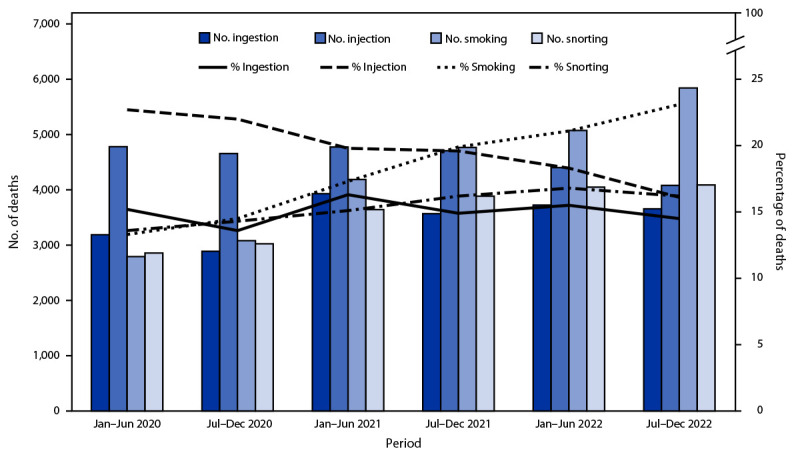
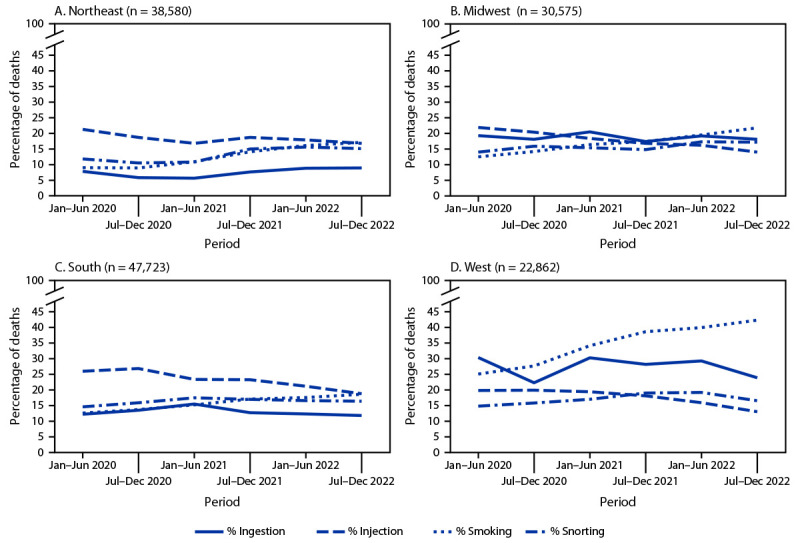
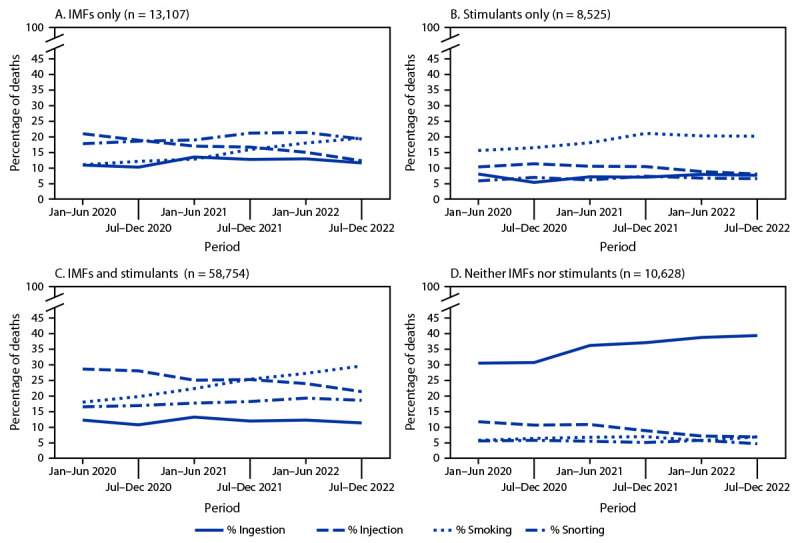
Preliminary reports indicate that more than 109,000 drug overdose deaths occurred in the United States in 2022; nearly 70% of these involved synthetic opioids other than methadone, primarily illegally manufactured fentanyl and fentanyl analogs (IMFs). Data from the western United States suggested a transition from injecting heroin to smoking IMFs. CDC analyzed data from the State Unintentional Drug Overdose Reporting System to describe trends in routes of drug use in 27 states and the District of Columbia among overdose deaths that occurred during January 2020-December 2022, overall and by region and drugs detected. From January-June 2020 to July-December 2022, the percentage of overdose deaths with evidence of injection decreased 29.1%, from 22.7% to 16.1%, whereas the percentage with evidence of smoking increased 73.7%, from 13.3% to 23.1%. The number of deaths with evidence of smoking increased 109.1%, from 2,794 to 5,843, and by 2022, smoking was the most commonly documented route of use in overdose deaths. Trends were similar in all U.S. regions. Among deaths with only IMFs detected, the percentage with evidence of injection decreased 41.6%, from 20.9% during January-June 2020 to 12.2% during July-December 2022, whereas the percentage with evidence of smoking increased 78.9%, from 10.9% to 19.5%. Similar trends were observed among deaths with both IMFs and stimulants detected. Strengthening public health and harm reduction services to address overdose risk related to diverse routes of drug use, including smoking and other noninjection routes, might reduce drug overdose deaths.
Conflict of interest statement
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. No potential conflicts of interest were disclosed.
Figures
References
-
- Valasek CJ, Streuli SA, Pines HA, et al. “A lotta people switched playing hard ball to playing Russian roulette”: experiences with rising overdose incidence caused by drug supply changes during the COVID-19 pandemic in the San Diego-Tijuana border metroplex. Drug Alcohol Depend Rep 2023;7:100154. 10.1016/j.dadr.2023.100154 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
