

Stress-induced hyperglycemia is associated with the mortality of thrombotic thrombocytopenic purpura patients
- PMID: 38360738
- PMCID: PMC10870494
- DOI: 10.1186/s13098-024-01275-2
Stress-induced hyperglycemia is associated with the mortality of thrombotic thrombocytopenic purpura patients
Abstract
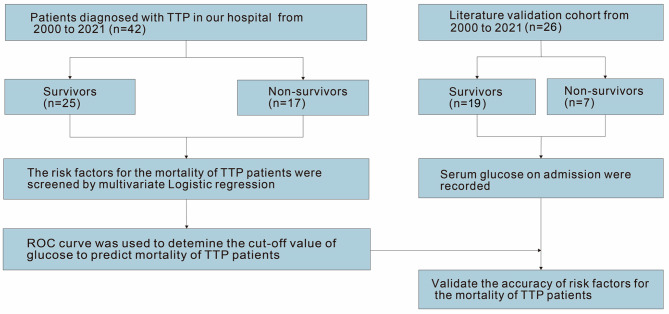
Background: Thrombotic thrombocytopenic purpura (TTP) is a rare thrombotic microangiopathy with a rapid progression and high mortality rate. We aimed to explore early risk factors for mortality in patients with TTP.
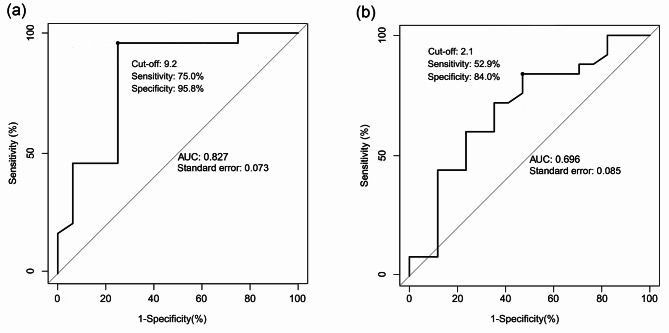
Methods: We conducted a retrospective analysis of 42 TTP patients that were admitted to our hospital between 2000 and 2021, with a median age of 49 (29-63) years. Risk factors for mortality were evaluated using multivariate logistic regression. Receiver operating characteristic curve analysis was used to determine the cut-off value of glucose for predicting mortality in patients, which was validated by comparison to a similar cohort in the published literature.
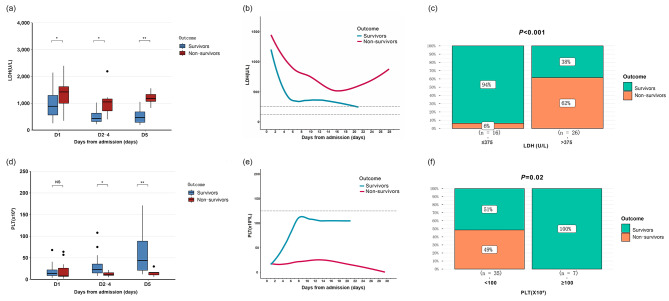
Results: Elevated glucose level and reduced red blood cells (RBC) counts were risk factors for mortality in patients with TTP (glucose, odds ratio and 95% confidence interval: 2.476 [1.368-4.484]; RBC, odds ratio and 95% confidence interval: 0.095 [0.011-0.799]). The area under the curve of glucose was 0.827, and the cut-off value was 9.2 mmol/L, with a sensitivity of 75.0% and specificity of 95.8%. A total of 26 cases from the validation cohort had a sensitivity of 71.0% and a specificity of 84.0%. The change trends of the TTP-related laboratory indices differed during hospitalization.
Conclusion: Hyperglycemia at admission and unstable blood glucose levels during hospitalization may be potential predictors of mortality for TTP patients. The improved prognosis was associated with the recovery of platelet counts and a significant decrease in serum lactate dehydrogenase after five days of treatment.
Keywords: Lactate dehydrogenase; Platelet; Prognosis; Thrombotic thrombocytopenic purpura.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing financial interests.
Figures


References
-
- George JN. Clinical practice. Thrombotic Thrombocytopenic Purpura. N Engl J Med. 2006;354(18):1927–35. 10.1056/NEJMcp053024. IF: 158.5 Q1 B1 IF: 158.5 Q1 B1 IF: 158.5 Q1 B1 IF: 158.5 Q1 B1 IF: 158.5 Q1 B1 IF: 158.5 Q1 B1 IF: 158.5 Q1 B1. Epub 2006/05/05. - PubMed
-
- Kremer Hovinga JA, Coppo P, Lammle B, Moake JL, Miyata T, Vanhoorelbeke K. Thrombotic Thrombocytopenic Purpura. Nat Rev Dis Primers (2017) 3:17020. Epub 2017/04/07. 10.1038/nrdp.2017.20. IF: 81.5 Q1 B1 IF: 81.5 Q1 B1 IF: 81.5 Q1 B1 IF: 81.5 Q1 B1 IF: 81.5 Q1 B1 IF: 81.5 Q1 B1 IF: 81.5 Q1 B1. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
