

Prediction of esophagogastroduodenoscopy therapeutic usefulness for in-ICU suspected upper gastrointestinal bleeding: the SUGIBI score study
- PMID: 38361004
- PMCID: PMC10869326
- DOI: 10.1186/s13613-024-01250-0
Prediction of esophagogastroduodenoscopy therapeutic usefulness for in-ICU suspected upper gastrointestinal bleeding: the SUGIBI score study
Abstract
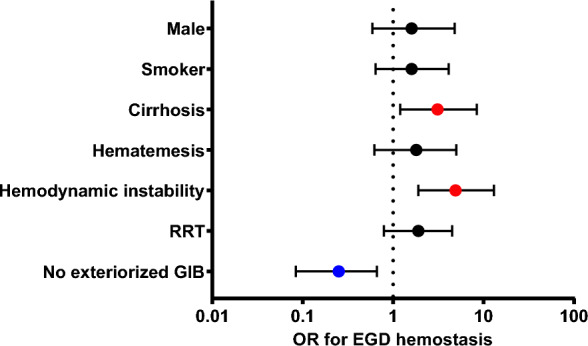
Background: Suspected upper gastrointestinal bleeding (SUGIB) is a common issue during ICU stay. In the absence of specific guidelines on the indication and timing of esophagogastroduodenoscopy (EGD), there is substantial variability in EGD indication depending on accessibility and clinical presentation. This study aimed to investigate factors associated with the need for per-EGD hemostatic therapy and to create a score predicting therapeutic benefit of emergency bedside EGD in ICU patients with SUGIB.
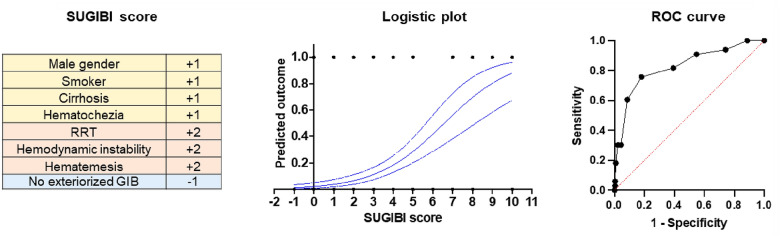
Methods: We conducted a retrospective study in our ICU to identify factors associated with the need for hemostatic procedure during EGD performed for SUGIB. From this observational cohort, we derived a score predicting the need for hemostasis during EGD, the SUGIBI score. This score was subsequently validated in a retrospective multicenter cohort.
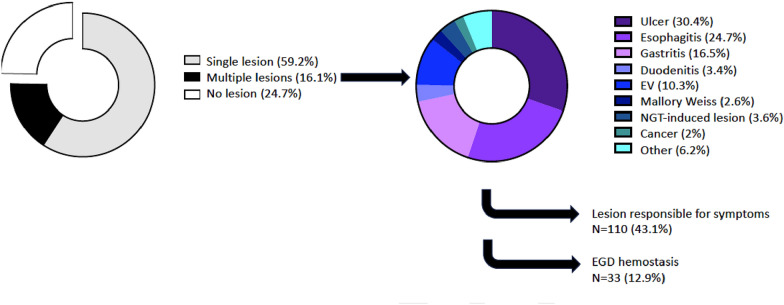
Results: Two hundred fifty-five patients not primarily admitted for GI bleeding who underwent a bedside EGD for SUGIB during their ICU stay were analyzed. The preeminent EGD indication were anemia (79%), melena (19%), shock (14%), and hematemesis (13%). EGD was normal in 24.7% of cases, while primary lesions reported were ulcers (23.1%), esophagitis (18.8%), and gastritis (12.5%). Only 12.9% of patients underwent hemostatic endotherapy during EGD. A SUGIBI score < 4 had a negative predictive value of 95% (91-99) for hemostatic endotherapy [AUC of 0.81; 0.75-0.91 (p < 0.0001)]. The SUGIBI score for predicting the need for an EGD-guided hemostatic procedure was next validated in a multicenter cohort with an AUC of 0.75 (0.66-0.85) (p < 0.0001), a score < 4 having a negative predictive value of 95% (92-97).
Conclusions: Our study shows that the therapeutic usefulness of bedside emergency EGD for SUGIB in critically ill patients is limited to a minority of patients. The SUGIBI score should help clinicians stratify the probability of a therapeutic EGD.
Keywords: Endotherapy; Esophagogastroduodenoscopy; Gastrointestinal bleeding; Hemostasis; «Stress» ulcer.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Cook D, Heyland D, Griffith L, Cook R, Marshall J, Pagliarello J, Canadian Critical Care Trials Group Risk factors for clinically important upper gastrointestinal bleeding in patients requiring mechanical ventilation. Crit Care Med. 1999;27(12):2812–2817. doi: 10.1097/00003246-199912000-00034. - DOI - PubMed
LinkOut - more resources
Full Text Sources
