

Pregnancy and cardiac maternal outcomes in women with inherited cardiomyopathy: interest of the CARPREG II risk score
- PMID: 38361389
- PMCID: PMC11098662
- DOI: 10.1002/ehf2.14694
Pregnancy and cardiac maternal outcomes in women with inherited cardiomyopathy: interest of the CARPREG II risk score
Abstract
Aims: Inherited cardiomyopathies are relatively rare but carry a high risk of cardiac maternal morbidity and mortality during pregnancy and postpartum. However, data for risk stratification are scarce. The new CARPREG II score improves prediction of prognosis in pregnancies associated with heart disease, though its role in inherited cardiomyopathies is unclear. We aim to describe characteristics and cardiac maternal outcomes in patients with inherited cardiomyopathy during pregnancy, and to evaluate the interest of the CARPREG II risk score in this population.
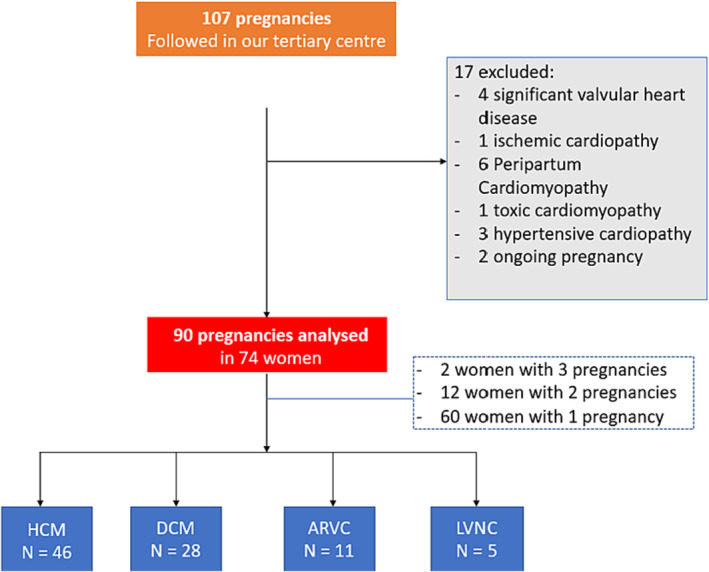
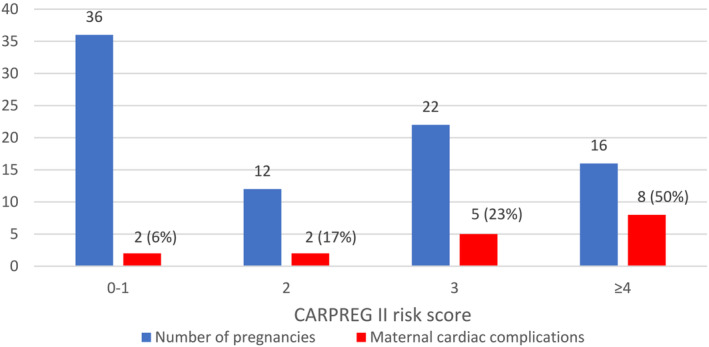
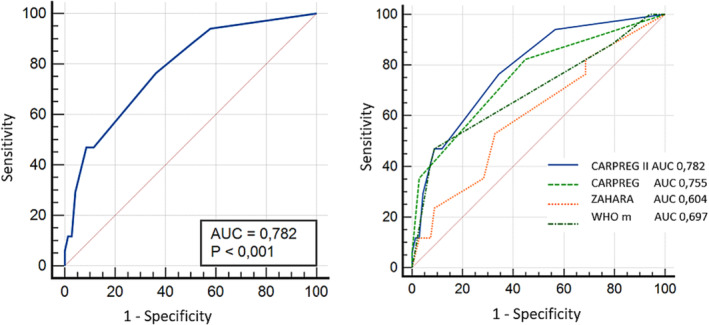
Methods and results: In this retrospective single-centre study, 90 consecutive pregnancies in 74 patients were included (mean age 32 ± 5 years), including 28 cases of dilated cardiomyopathy (DCM), 46 of hypertrophic cardiomyopathy, 11 of arrhythmogenic right ventricular cardiomyopathy and 5 of left ventricular noncompaction, excluding peripartum cardiomyopathy. The discriminatory power of several risk scores was assessed by the area under the receiver-operating characteristic curve (AUC). Median CARPREG II score was 2 [0;3] and was higher in the DCM subgroup. A severe cardiac maternal complication was observed in 18 (20%) pregnancies, mainly driven by arrhythmia and heart failure (each event in 10 pregnancies), with 3 cardiovascular deaths. Forty-three pregnancies (48%) presented foetal/neonatal complications (18 premature delivery, 3 foetal/neonatal death). CARPREG II was significantly associated with cardiac maternal complications (P < 0.05 for all) and showed a higher AUC (0.782) than CARPREG (0.755), mWHO (0.697) and ZAHARA (0.604).
Conclusions: Pregnancy in women with inherited cardiomyopathy carries a high risk of maternal cardiovascular complications. CARPREG II is the most efficient predictor of cardiovascular complications in this population.
Keywords: Cardiomyopathy; Pregnancy; Prognosis; Risk score.
© 2024 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared in relation to this work. Estelle Gandjbakhch reported consulting/educational and presentation fees, not related to the present work, from medtronic/boston: abbott/zoll.
Figures
References
-
- Roos‐Hesselink J, Baris L, Johnson M, De Backer J, Otto C, Marelli A, et al. Pregnancy outcomes in women with cardiovascular disease: Evolving trends over 10 years in the ESC Registry Of Pregnancy And Cardiac disease (ROPAC). Eur Heart J 2019;40:3848‐3855. doi:10.1093/eurheartj/ehz136 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
