

Comparison of Remotely Applied and Face-to-Face Disease Activity Scores in Saudi Arabian Patients With Rheumatoid Arthritis: A Prospective Cohort Study
- PMID: 38361704
- PMCID: PMC10868911
- DOI: 10.7759/cureus.52390
Comparison of Remotely Applied and Face-to-Face Disease Activity Scores in Saudi Arabian Patients With Rheumatoid Arthritis: A Prospective Cohort Study
Abstract
Objectives: This study aimed to assess the disease activity indices (DAI) of rheumatoid arthritis (RA) by telephone-based tele-visits compared to face-to-face clinic encounters.
Methods: Patients with RA attending outpatient clinics between December 2021 and May 2022 were prospectively recruited. Disease activity assessments were initially performed in the clinic using the disease activity score 28-C-reactive protein (DAS28-CRP) and disease activity score 28-erythrocyte sedimentation rate (DAS28-ESR). Within two weeks of the clinic visit, a telephone-based assessment gathered information on demographics, Routine Assessment of Patient Index Data 3 (RAPID3) score, and satisfaction. Disease activity scores were dichotomized into remission or low disease activity and moderate to high disease activity.
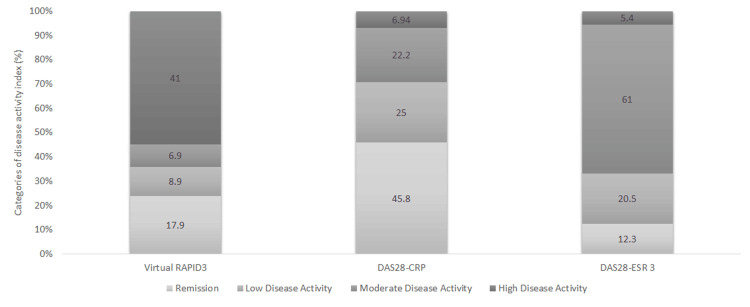
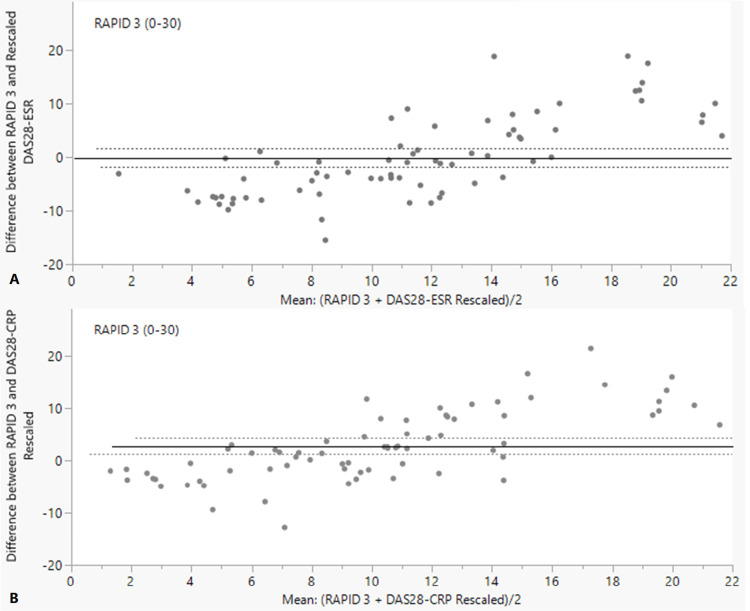
Results: A total of 78 patients completed the two-point interview. Of those, 62 (79.49%) were women, with a mean age of 54.73±13.71 years. Seropositivity for rheumatoid factor and/or anti-citrullinated peptide was observed in 51 (83.61%) participants. Twenty-seven percent of the patients were classified as in remission or low disease activity by RAPID3. This was 71% for DAS28-CRP and 33% for DAS28-ESR. Based on the dichotomized disease activity classification, the agreement percentage between RAPID3 and DAS28-ESR was 78.08%, while it was 47.22% between RAPID3 and DAS28-CRP, which resulted in kappa statistic values of 0.48 (moderate agreement) and 0.14 (low agreement), respectively. Satisfaction rates were low.
Conclusion: Telephone-based RAPID3 showed a low-moderate agreeability compared to DAS28 and had low satisfaction rates. This suggests that tele-rheumatology care by this means was not feasible for following up with patients with RA and warrants further development.
Keywords: covid-19; disease activity in rheumatoid arthritis; patients satisfaction; saudi arabia; telemedicine.
Copyright © 2024, Almansouri et al.
Conflict of interest statement
A license agreement from the copyright author of the RAPID3 score, Dr. Theodore Pincus, was obtained for our study, in agreement with RWS Life Sciences.
Figures
Similar articles
-
Correlation of Disease Activity Scores and Routine Assessment of Patient Index Data (RAPID3) on a Multidimensional Health Assessment Questionnaire in Patients With Rheumatoid Arthritis: A Saudi Experience.Cureus. 2023 Sep 10;15(9):e44982. doi: 10.7759/cureus.44982. eCollection 2023 Sep. Cureus. 2023. PMID: 37822428 Free PMC article.
-
Comparison of Disease Activity Score in 28 joints with ESR (DAS28), Clinical Disease Activity Index (CDAI), Health Assessment Questionnaire Disability Index (HAQ-DI) & Routine Assessment of Patient Index Data with 3 measures (RAPID3) for assessing disease activity in patients with rheumatoid arthritis at initial presentation.Indian J Med Res. 2017 Nov;146(Supplement):S57-S62. doi: 10.4103/ijmr.IJMR_701_15. Indian J Med Res. 2017. PMID: 29578196 Free PMC article.
-
The RAPID3 questionnaire as a screening tool to reduce the number of outpatient clinic visits: a retrospective cohort study.Clin Rheumatol. 2022 Aug;41(8):2525-2531. doi: 10.1007/s10067-022-06162-7. Epub 2022 Apr 26. Clin Rheumatol. 2022. PMID: 35469354 Free PMC article.
-
Can RAPID3, an index without formal joint counts or laboratory tests, serve to guide rheumatologists in tight control of rheumatoid arthritis in usual clinical care?Bull NYU Hosp Jt Dis. 2009;67(3):254-66. Bull NYU Hosp Jt Dis. 2009. PMID: 19852747 Review.
-
RAPID3, an index to assess and monitor patients with rheumatoid arthritis, without formal joint counts: similar results to DAS28 and CDAI in clinical trials and clinical care.Rheum Dis Clin North Am. 2009 Nov;35(4):773-8, viii. doi: 10.1016/j.rdc.2009.10.008. Rheum Dis Clin North Am. 2009. PMID: 19962621 Review.
References
-
- Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. van Prevoo ML, van ’t Hof MA, Kuper HH, van Leeuwen MA, van de Putte LB, van Riel PL. Arthritis Rheum. 1995;38:44–48. - PubMed
-
- RAPID3 (Routine Assessment of Patient Index Data 3), a rheumatoid arthritis index without formal joint counts for routine care: proposed severity categories compared to disease activity score and clinical disease activity index categories. Pincus T, Swearingen CJ, Bergman M, Yazici Y. J Rheumatol. 2008;35:2136–2147. - PubMed
-
- Comparison of Disease Activity Score in 28 joints with ESR (DAS28), Clinical Disease Activity Index (CDAI), Health Assessment Questionnaire Disability Index (HAQ-DI) & Routine Assessment of Patient Index Data with 3 measures (RAPID3) for assessing disease activity in patients with rheumatoid arthritis at initial presentation. Kumar BS, Suneetha P, Mohan A, Kumar DP, Sarma KVS. Indian J Med Res. 2017;146:57. - PMC - PubMed
-
- Correlation between rapid-3, DAS28, CDAI and SDAI as a measure of disease activity in a cohort of Colombian patients with rheumatoid arthritis. Muñoz JGB, Giraldo RB, Santos AM, et al. Clin Rheumatol. 2017;36:1143–1148. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous