

Aspergillus granulosus femoral osteomyelitis in a cardiac transplant patient: first reported case and literature review
- PMID: 38361916
- PMCID: PMC10868480
- DOI: 10.1177/20499361241231482
Aspergillus granulosus femoral osteomyelitis in a cardiac transplant patient: first reported case and literature review
Abstract
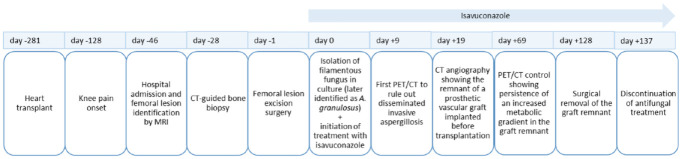
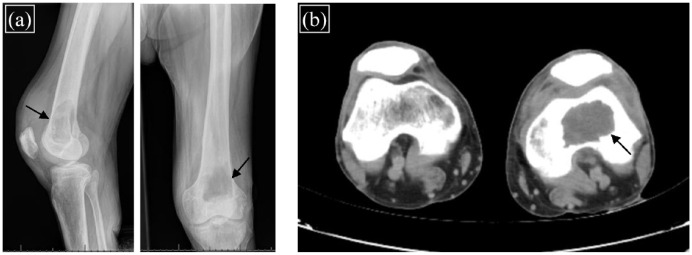
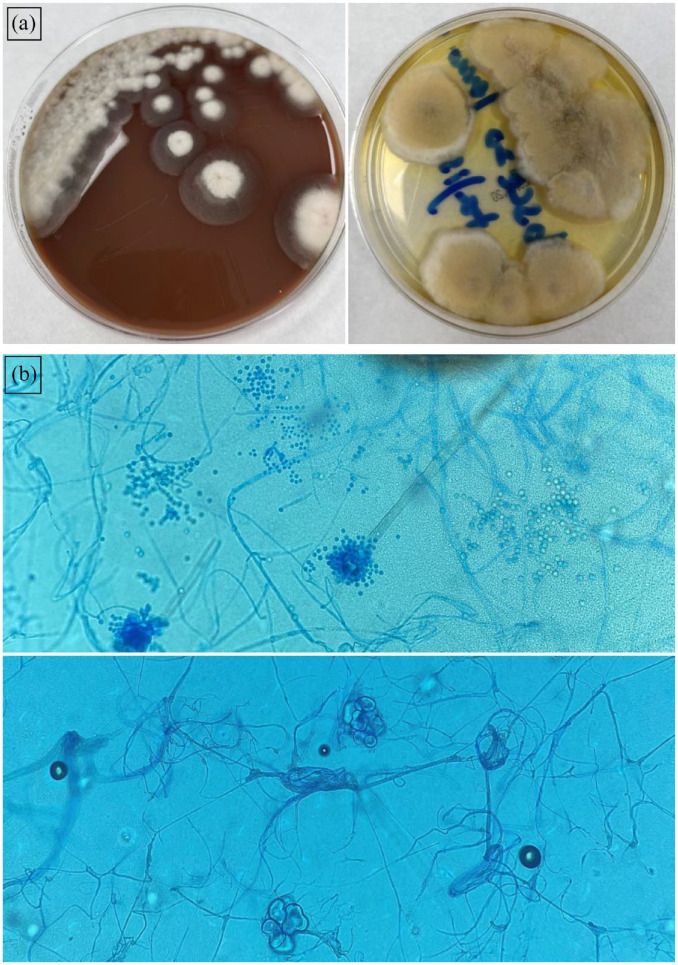
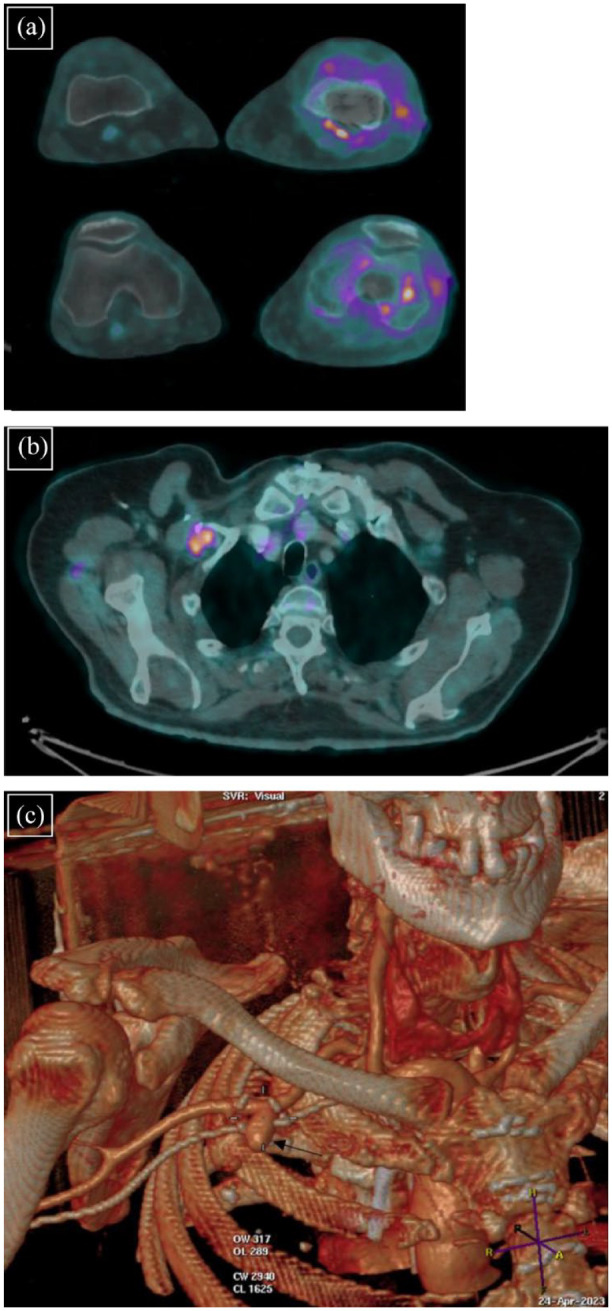
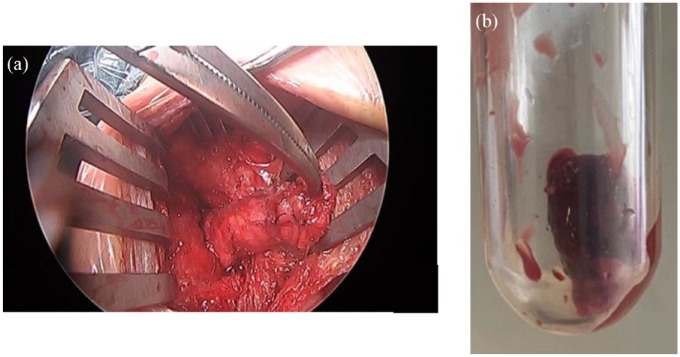
Aspergillus osteomyelitis is a rare complication of extrapulmonary invasive aspergillosis, which usually presents as spondylodiscitis. The clinical picture is usually paucisymptomatic and of long evolution, which leads to diagnostic difficulties, especially in immunosuppressed patients presenting a delayed systemic host response. We report a case of femoral osteomyelitis caused by Aspergillus granulosus in a heart transplant recipient successfully treated with a combined surgical and antifungal approach. A 65-year-old heart transplant male presented with left knee pain lasting 3 months. X-ray and magnetic resonance imaging identified a lesion with aggressive characteristics at the distal third of the left femur, due to which the patient underwent excisional surgery. Aspergillus granulosus was cultured from the removed material and antifungal treatment with oral isavuconazole was started. Chest imaging excluded pulmonary aspergillosis, while the positron emission tomography/computed tomography (PET/CT) identified a remnant of a prosthetic vascular graft sewn to the proximal third of the right axillary artery, through which a catheter-based micro-axial left ventricular assist device was implanted previously as bridge to transplant therapy. The patient presented a rapid clinical improvement with complete functional recovery following the surgical treatment and the antifungal therapy and finally underwent surgical removal of the residual vascular graft. This is the first reported episode of long bone osteomyelitis due to A. granulosus that occurred in a heart transplant recipient without pulmonary infection and was successfully treated with isavuconazole. The PET/CT was useful in supporting the diagnostic process and follow-up. Cryptic fungal species can cause invasive infections, particularly in immunocompromised patients. Molecular methods are crucial in fungal identification.
Keywords: Aspergillus granulosus; case report; heart transplantation; invasive aspergillosis; invasive fungal infection; osteomyelitis; solid organ transplantation.
© The Author(s), 2024.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
Similar articles
-
Aspergillosis Osteomyelitis of the Mandible: A Case Report and Literature Review.Sage Open Pathol. 2025 May 29;18:30502098251344770. doi: 10.1177/30502098251344770. eCollection 2025 Jan-Dec. Sage Open Pathol. 2025. PMID: 40519329 Free PMC article.
-
Aspergillus terreus spondylodiscitis following an abdominal stab wound: a case report.J Med Case Rep. 2019 Jun 5;13(1):172. doi: 10.1186/s13256-019-2109-5. J Med Case Rep. 2019. PMID: 31164170 Free PMC article.
-
Aspergillus Osteomyelitis of the Ribs in Immunocompetent Hosts: Report of Two Rare Cases.J Orthop Case Rep. 2017 Jul-Aug;7(4):61-64. doi: 10.13107/jocr.2250-0685.854. J Orthop Case Rep. 2017. PMID: 29181357 Free PMC article.
-
Isavuconazole in the Treatment of Aspergillus fumigatus Fracture-Related Infection: Case Report and Literature Review.Antibiotics (Basel). 2022 Mar 5;11(3):344. doi: 10.3390/antibiotics11030344. Antibiotics (Basel). 2022. PMID: 35326807 Free PMC article. Review.
-
Invasive aspergillosis in liver transplant recipients.Transpl Infect Dis. 2023 Jun;25(3):e14049. doi: 10.1111/tid.14049. Epub 2023 Mar 16. Transpl Infect Dis. 2023. PMID: 36929539 Review.
Cited by
-
Update on invasive fungal infections: emerging trends in the incidence of fungal infections in immunosuppressed patients and associated conditions.Ther Adv Infect Dis. 2024 Sep 27;11:20499361241282835. doi: 10.1177/20499361241282835. eCollection 2024 Jan-Dec. Ther Adv Infect Dis. 2024. PMID: 39376744 Free PMC article. No abstract available.
References
-
- Segal BH. Aspergillosis. N Engl J Med 2009; 360: 1870–1884. - PubMed
-
- Ben-Ami R, Lewis RE, Kontoyiannis DP. Enemy of the (immunosuppressed) state: an update on the pathogenesis of Aspergillus fumigatus infection. Br J Haematol 2010; 150: 406–417. - PubMed
-
- Horn D, Sae-Tia S, Neofytos D. Aspergillus osteomyelitis: review of 12 cases identified by the Prospective Antifungal Therapy Alliance registry. Diagn Microbiol Infect Dis 2009; 63: 384–387. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
