

Selective sodium-glucose cotransporter-2 inhibitors in the improvement of hemoglobin and hematocrit in patients with type 2 diabetes mellitus: a network meta-analysis
- PMID: 38362282
- PMCID: PMC10867125
- DOI: 10.3389/fendo.2024.1333624
Selective sodium-glucose cotransporter-2 inhibitors in the improvement of hemoglobin and hematocrit in patients with type 2 diabetes mellitus: a network meta-analysis
Abstract
Objective: To compare the effects of different selective sodium-glucose cotransporter-2 inhibitors (SGLT2i) on hemoglobin and hematocrit in patients with type 2 diabetes mellitus (T2DM) with a network meta-analysis (NMA).
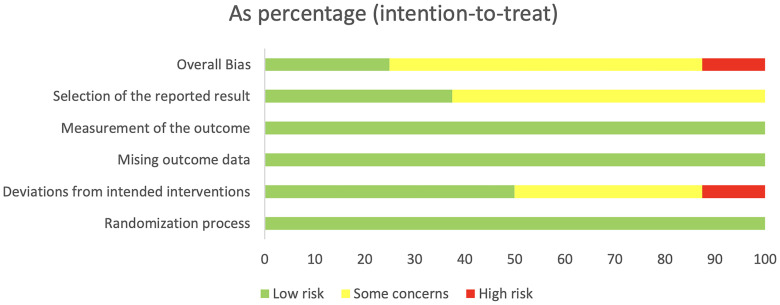
Methods: Randomized controlled trials (RCTs) on SGLT2i for patients with T2DM were searched in PubMed, Embase, Cochrane Library, and Web of Science from inception of these databases to July 1, 2023. The risk of bias (RoB) tool was used to evaluate the quality of the included studies, and R software was adopted for data analysis.
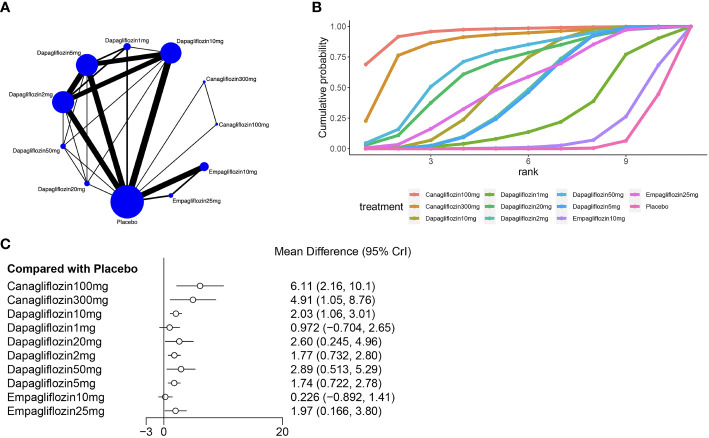
Results: Twenty-two articles were included, involving a total of 14,001 T2DM patients. SGLT2i included empagliflozin, dapagliflozin, and canagliflozin. The NMA results showed that compared with placebo, canagliflozin 100mg, canagliflozin 300mg, dapagliflozin 10mg, dapagliflozin 2mg, dapagliflozin 50mg, dapagliflozin 5mg, empagliflozin 25mg, and dapagliflozin 20mg increased hematocrit in patients with T2DM, while canagliflozin 100mg, canagliflozin 200mg, canagliflozin 300mg increased hemoglobin in patients with T2DM. In addition, the NMA results indicated that canagliflozin 100mg had the best effect on the improvement of hematocrit, and canagliflozin 200mg had the best effect on the improvement of hemoglobin.
Conclusion: Based on the existing studies, we concluded that SGLT2i could increase hematocrit and hemoglobin levels in patients with T2DM, and canagliflozin 100mg had the best effect on the improvement of hematocrit, while canagliflozin 200mg had the best effect on the improvement of hemoglobin.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/#loginpage, identifier PROSPERO (CRD42023477103).
Keywords: hematocrit; hemoglobin; network meta; selective sodium-glucose cotransporter-2 inhibitor; type 2 diabetes mellitus.
Copyright © 2024 Luo, Bai, Zhang and Qin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Comparative safety of different recommended doses of sodium-glucose cotransporter 2 inhibitors in patients with type 2 diabetes mellitus: a systematic review and network meta-analysis of randomized clinical trials.Front Endocrinol (Lausanne). 2023 Nov 10;14:1256548. doi: 10.3389/fendo.2023.1256548. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 38027214 Free PMC article.
-
Comparative cardiovascular benefits of individual SGLT2 inhibitors in type 2 diabetes and heart failure: a systematic review and network meta-analysis of randomized controlled trials.Front Endocrinol (Lausanne). 2023 Dec 20;14:1216160. doi: 10.3389/fendo.2023.1216160. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 38179304 Free PMC article.
-
Evaluating the costs of glycemic response with canagliflozin versus dapagliflozin and empagliflozin as add-on to metformin in patients with type 2 diabetes mellitus in the United Arab Emirates.Curr Med Res Opin. 2017 Jun;33(6):1155-1163. doi: 10.1080/03007995.2017.1310091. Epub 2017 Apr 28. Curr Med Res Opin. 2017. PMID: 28323512
-
Urinary tract and genital infections in patients with type 2 diabetes treated with sodium-glucose co-transporter 2 inhibitors: A meta-analysis of randomized controlled trials.Diabetes Obes Metab. 2017 Mar;19(3):348-355. doi: 10.1111/dom.12825. Epub 2016 Dec 19. Diabetes Obes Metab. 2017. PMID: 27862830
-
Comparative safety of different sodium-glucose transporter 2 inhibitors in patients with type 2 diabetes: a systematic review and network meta-analysis of randomized controlled trials.Front Endocrinol (Lausanne). 2023 Aug 28;14:1238399. doi: 10.3389/fendo.2023.1238399. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37701900 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical