

Continuous glucose monitoring in adults with type 2 diabetes: a systematic review and meta-analysis
- PMID: 38363342
- PMCID: PMC10954850
- DOI: 10.1007/s00125-024-06107-6
Continuous glucose monitoring in adults with type 2 diabetes: a systematic review and meta-analysis
Abstract
Aims/hypothesis: Continuous glucose monitoring (CGM) is increasingly used in the treatment of type 2 diabetes, but the effects on glycaemic control are unclear. The aim of this systematic review and meta-analysis is to provide a comprehensive overview of the effect of CGM on glycaemic control in adults with type 2 diabetes.
Methods: We performed a systematic review using Embase, MEDLINE, Web of Science, Scopus and ClinicalTrials.gov from inception until 2 May 2023. We included RCTs investigating real-time CGM (rtCGM) or intermittently scanned CGM (isCGM) compared with self-monitoring of blood glucose (SMBG) in adults with type 2 diabetes. Studies with an intervention duration <6 weeks or investigating professional CGM, a combination of CGM and additional glucose-lowering treatment strategies or GlucoWatch were not eligible. Change in HbA1c and the CGM metrics time in range (TIR), time below range (TBR), time above range (TAR) and glycaemic variability were extracted. We evaluated the risk of bias using the Cochrane risk-of-bias tool version 2. Data were synthesised by performing a meta-analysis. We also explored the effects of CGM on severe hypoglycaemia and micro- and macrovascular complications.
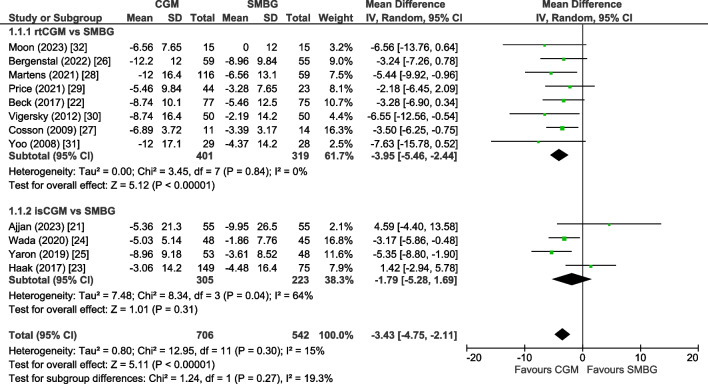
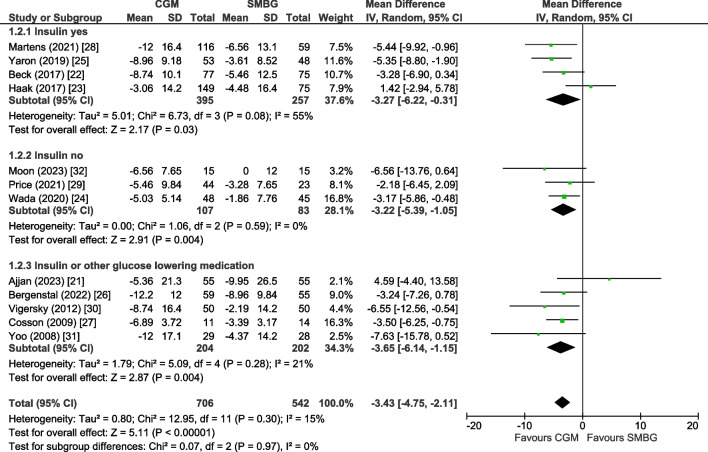
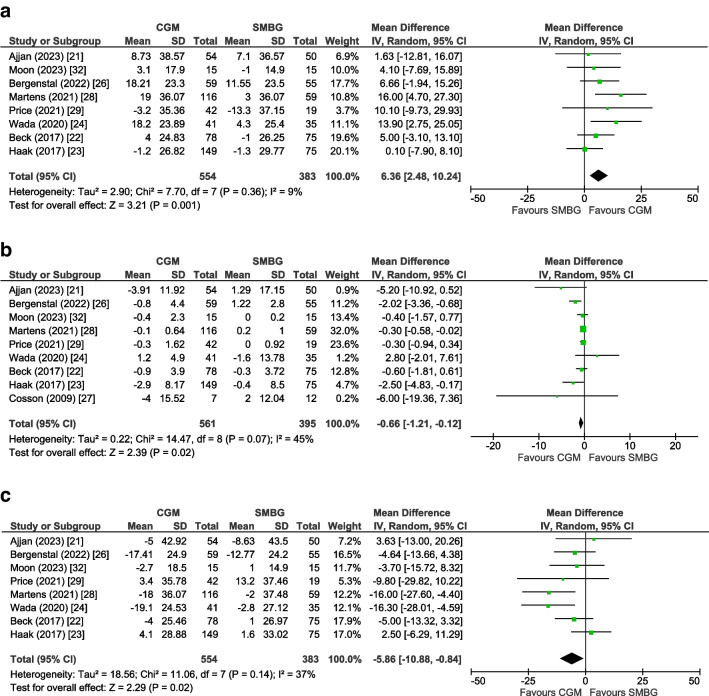
Results: We found 12 RCTs comprising 1248 participants, with eight investigating rtCGM and four isCGM. Compared with SMBG, CGM use (rtCGM or isCGM) led to a mean difference (MD) in HbA1c of -3.43 mmol/mol (-0.31%; 95% CI -4.75, -2.11, p<0.00001, I2=15%; moderate certainty). This effect was comparable in studies that included individuals using insulin with or without oral agents (MD -3.27 mmol/mol [-0.30%]; 95% CI -6.22, -0.31, p=0.03, I2=55%), and individuals using oral agents only (MD -3.22 mmol/mol [-0.29%]; 95% CI -5.39, -1.05, p=0.004, I2=0%). Use of rtCGM showed a trend towards a larger effect (MD -3.95 mmol/mol [-0.36%]; 95% CI -5.46 to -2.44, p<0.00001, I2=0%) than use of isCGM (MD -1.79 mmol/mol [-0.16%]; 95% CI -5.28, 1.69, p=0.31, I2=64%). CGM was also associated with an increase in TIR (+6.36%; 95% CI +2.48, +10.24, p=0.001, I2=9%) and a decrease in TBR (-0.66%; 95% CI -1.21, -0.12, p=0.02, I2=45%), TAR (-5.86%; 95% CI -10.88, -0.84, p=0.02, I2=37%) and glycaemic variability (-1.47%; 95% CI -2.94, -0.01, p=0.05, I2=0%). Three studies reported one or more events of severe hypoglycaemia and macrovascular complications. In comparison with SMBG, CGM use led to a non-statistically significant difference in the incidence of severe hypoglycaemia (RR 0.66, 95% CI 0.15, 3.00, p=0.57, I2=0%) and macrovascular complications (RR 1.54, 95% CI 0.42, 5.72, p=0.52, I2=29%). No trials reported data on microvascular complications.
Conclusions/interpretation: CGM use compared with SMBG is associated with improvements in glycaemic control in adults with type 2 diabetes. However, all studies were open label. In addition, outcome data on incident severe hypoglycaemia and incident microvascular and macrovascular complications were scarce.
Registration: This systematic review was registered on PROSPERO (ID CRD42023418005).
Keywords: CGM; Continuous glucose monitoring; Glycaemic control; Meta-analysis; Systematic review; Type 2 Diabetes.
© 2024. The Author(s).
Figures
Comment in
-
CGM verbessert Werte auch bei leichterem Typ-2-Diabetes.MMW Fortschr Med. 2024 Oct;166(18):24-26. doi: 10.1007/s15006-024-4379-0. MMW Fortschr Med. 2024. PMID: 39448474 Review. German. No abstract available.
References
-
- Davies MJ, Aroda VR, Collins BS, et al. Management of hyperglycaemia in type 2 diabetes, 2022. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD) Diabetologia. 2022;65:1925–1966. doi: 10.1007/s00125-022-05787-2. - DOI - PMC - PubMed
-
- Czupryniak L, Barkai L, Bolgarska S, et al. Self-monitoring of blood glucose in diabetes: from evidence to clinical reality in Central and Eastern Europe - recommendations from the international Central-Eastern European expert group. Diabetes Technol Ther. 2014;16:460–475. doi: 10.1089/dia.2013.0302. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
