

Fully endoscopic microvascular decompression for hemifacial spasm: a clinical study and analysis
- PMID: 38363437
- PMCID: PMC10873216
- DOI: 10.1007/s10143-024-02311-5
Fully endoscopic microvascular decompression for hemifacial spasm: a clinical study and analysis
Abstract
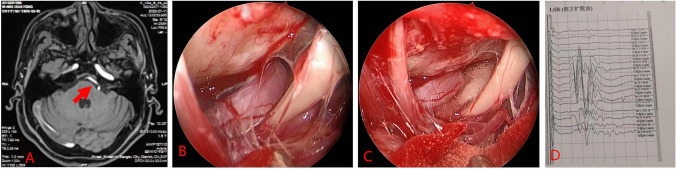
Fully endoscopic microvascular decompression (MVD) of the facial nerve is the main surgical treatment for hemifacial spasm. However, the technique presents distinct surgical challenges. We retrospectively analyzed prior cases to consolidate surgical insights and assess clinical outcomes. Clinical data from 16 patients with facial nerve spasms treated at the Department of Neurosurgery in the First Affiliated Hospital of Bengbu Medical College, between August 2020 and July 2023, were retrospectively examined. Preoperatively, all patients underwent magnetic resonance angiography to detect any offending blood vessels; ascertain the relationship between offending vessels, facial nerves, and the brainstem; and detect any cerebellopontine angle lesions. Surgery involved endoscopic MVD of the facial nerve using a mini Sigmoid sinus posterior approach. Various operative nuances were summarized and analyzed, and clinical efficacy, including postoperative complications and the extent of relief from facial paralysis, was evaluated. Fully endoscopic MVD was completed in all patients, with the offending vessels identified and adequately padded during surgery. The offending vessels were anterior inferior cerebellar artery in 12 cases (75%), vertebral artery in 3 cases (18.75%), and posterior inferior cerebellar artery in 1 case (6.25%). Intraoperative electrophysiological monitoring revealed that the lateral spread response of the facial nerve vanished in 15 cases and remained unchanged in 1 case. Postoperative facial spasms were promptly alleviated in 15 cases (93.75%) and delayed in 1 case (6.25%). Two cases of postoperative complications were recorded-one intracranial infection and one case of tinnitus-both were resolved or mitigated with treatment. All patients were subject to follow-up, with no instances of recurrence or mortality. Fully endoscopic MVD of the facial nerve is safe and effective. Proficiency in endoscopy and surgical skills are vital for performing this procedure.
Keywords: Endoscope; Facial spasm; Microvascular decompression; Neuroendoscopy.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
MeSH terms
LinkOut - more resources
Full Text Sources
