

Asymptomatic uterine perforation and IUD migration to the broad ligament: A case report
- PMID: 38363896
- PMCID: PMC10869031
- DOI: 10.1097/MD.0000000000033857
Asymptomatic uterine perforation and IUD migration to the broad ligament: A case report
Abstract
Rationale: Uterine perforation is a serious complication of intrauterine contraceptive device (IUD) placement. However, as complete uterine perforation and extrauterine migration may remain asymptomatic, thorough localization of the IUD is important prior to reinsertion.
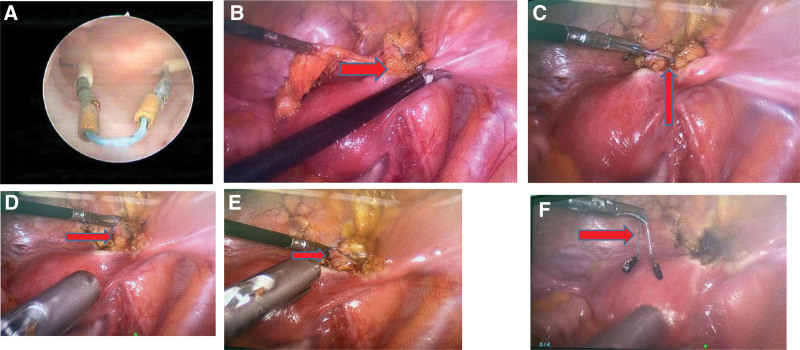
Patient concerns: A 33-year-old patient who has had 4 IUD insertions, wherein the location of the first IUD (inserted 14 years ago) was not identified prior to reinsertion and replacement of the subsequent three. She presented to hospital with a 6-month history of abdominal pain. Pelvic ultrasonography (US), radiography, hysteroscopy and laparoscopy examinations confirmed that a retained migrated IUD in the right broad ligament.
Diagnosis: Uterine perforation, IUD migration to the broad ligament.
Interventions: The patient underwent hysteroscopy and laparoscopy.
Outcomes: Both IUDs were successfully removed without any complications.
Copyright © 2024 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

Similar articles
-
Uterine perforation by copper intrauterine device.Eur J Obstet Gynecol Reprod Biol. 1984 Jun;17(4):257-61. doi: 10.1016/0028-2243(84)90068-6. Eur J Obstet Gynecol Reprod Biol. 1984. PMID: 6378687
-
Translocation of the Dalkon Shield into the broad ligament.Obstet Gynecol. 1975 Aug;46(2):239-42. Obstet Gynecol. 1975. PMID: 1171420
-
Dislocated intrauterine devices: clinical presentations, diagnosis and management.Eur J Contracept Reprod Health Care. 2021 Apr;26(2):160-166. doi: 10.1080/13625187.2021.1874337. Epub 2021 Feb 8. Eur J Contracept Reprod Health Care. 2021. PMID: 33555216
-
Complete and partial uterine perforation and embedding following insertion of intrauterine devices. II. Diagnostic methods, prevention, and management.Obstet Gynecol Surv. 1981 Aug;36(8):401-17. doi: 10.1097/00006254-198108000-00001. Obstet Gynecol Surv. 1981. PMID: 6455610 Review.
-
Vesical transmigration of an intrauterine contraceptive device: A rare case report and literature review.Medicine (Baltimore). 2017 Oct;96(40):e8236. doi: 10.1097/MD.0000000000008236. Medicine (Baltimore). 2017. PMID: 28984781 Free PMC article. Review.
Cited by
-
Migrated intra-uterine device to infra-umbilical skin: a rare case report.BMC Womens Health. 2024 Dec 30;24(1):672. doi: 10.1186/s12905-024-03522-0. BMC Womens Health. 2024. PMID: 39736668 Free PMC article.
References
-
- Zeyi C. Chinese Gynecology and Obstetrics: Volume 2. 3rd edn. Beijing, China: People’s Medical Publishing House; 2018:2932.
-
- Cetinkaya K, Kumtepe Y, Zngec M. Minimally invasive approach to cases of lost intra-uterine device: a 7-year experience. Eur J Obstet Gynecol Reprod Biol. 2011;159:119–21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
