

Pericardial effusion in oncological patients: current knowledge and principles of management
- PMID: 38365812
- PMCID: PMC10870633
- DOI: 10.1186/s40959-024-00207-3
Pericardial effusion in oncological patients: current knowledge and principles of management
Abstract
Background: This article provides an up-to-date overview of pericardial effusion in oncological practice and a guidance on its management. Furthermore, it addresses the question of when malignancy should be suspected in case of newly diagnosed pericardial effusion.
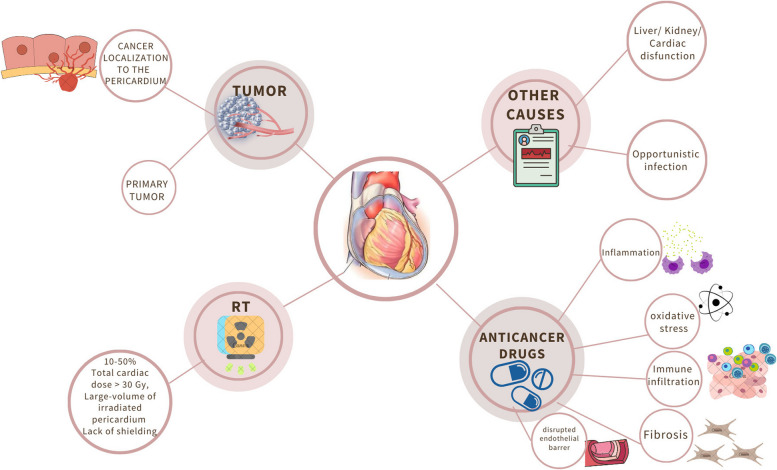
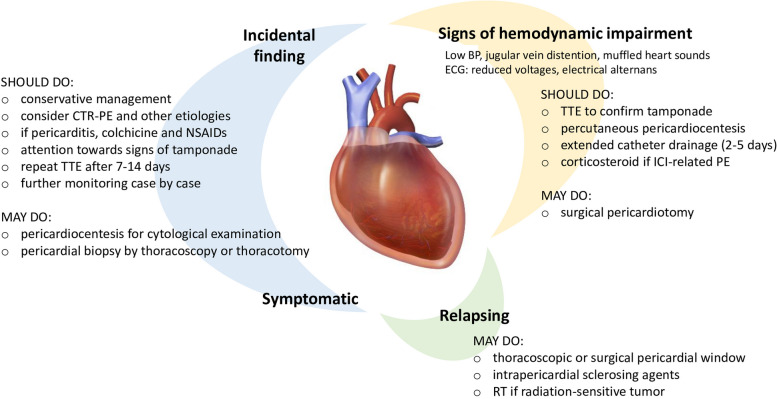
Main body: Cancer-related pericardial effusion is commonly the result of localization of lung and breast cancer, melanoma, or lymphoma to the pericardium via direct invasion, lymphatic dissemination, or hematogenous spread. Several cancer therapies may also cause pericardial effusion, most often during or shortly after administration. Pericardial effusion following radiation therapy may instead develop after years. Other diseases, such as infections, and, rarely, primary tumors of the pericardium complete the spectrum of the possible etiologies of pericardial effusion in oncological patients. The diagnosis of cancer-related pericardial effusion is usually incidental, but cancer accounts for approximately one third of all cardiac tamponades. Drainage, which is mainly attained by pericardiocentesis, is needed when cancer or cancer treatment-related pericardial effusion leads to hemodynamic impairment. Placement of a pericardial catheter for 2-5 days is advised after pericardial fluid removal. In contrast, even a large pericardial effusion should be conservatively managed when the patient is stable, although the best frequency and timing of monitoring by echocardiography in this context are yet to be established. Pericardial effusion secondary to immune checkpoint inhibitors typically responds to corticosteroid therapy. Pericardiocentesis may also be considered to confirm the presence of neoplastic cells in the pericardial fluid, but the yield of cytological examination is low. In case of newly found pericardial effusion in individuals without active cancer and/or recent cancer treatment, a history of malignancy, unremitting or recurrent course, large effusion or presentation with cardiac tamponade, incomplete response to empirical therapy with nonsteroidal anti-inflammatory, and hemorrhagic fluid at pericardiocentesis suggest a neoplastic etiology.
Keywords: Cancer; Cardio-oncology; Management.; Pericardiocentesis; Pericardium; Tamponade.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Intrapericardial cisplatin for the management of patients with large malignant pericardial effusion in the course of the lung cancer.Lung Cancer. 1997 Mar;16(2-3):215-22. doi: 10.1016/s0169-5002(96)00631-9. Lung Cancer. 1997. PMID: 9152952
-
Diagnosis of malignant pericarditis: a single centre experience.Kardiol Pol. 2012;70(11):1147-53. Kardiol Pol. 2012. PMID: 23180523
-
[Contrast medium echocardiography-assisted pericardial drainage].Herz. 2000 Dec;25(8):755-60. doi: 10.1007/pl00001994. Herz. 2000. PMID: 11200124 German.
-
Pericardial Effusions: Causes, Diagnosis, and Management.Prog Cardiovasc Dis. 2017 Jan-Feb;59(4):380-388. doi: 10.1016/j.pcad.2016.12.009. Epub 2017 Jan 4. Prog Cardiovasc Dis. 2017. PMID: 28062268 Review.
-
Management of pericardial effusion.Eur Heart J. 2013 Apr;34(16):1186-97. doi: 10.1093/eurheartj/ehs372. Epub 2012 Nov 2. Eur Heart J. 2013. PMID: 23125278 Review.
Cited by
-
Pericardial Disease in Patients with Cancer: Clinical Insights on Diagnosis and Treatment.Cancers (Basel). 2024 Oct 12;16(20):3466. doi: 10.3390/cancers16203466. Cancers (Basel). 2024. PMID: 39456560 Free PMC article. Review.
-
Impact of body mass index on in-hospital outcomes in patients receiving leadless pacemakers: A five-category analysis.Heart Rhythm O2. 2024 Oct 1;5(12):883-889. doi: 10.1016/j.hroo.2024.09.017. eCollection 2024 Dec. Heart Rhythm O2. 2024. PMID: 39803626 Free PMC article.
-
Incidence of secondary pericardial effusions associated with different etiologies: a comprehensive review of literature.J Cardiothorac Surg. 2025 Feb 22;20(1):141. doi: 10.1186/s13019-025-03370-5. J Cardiothorac Surg. 2025. PMID: 39987086 Free PMC article. Review.
-
Applications of Artificial Intelligence for the Prediction and Diagnosis of Cancer Therapy-Related Cardiac Dysfunction in Oncology Patients.Cancers (Basel). 2025 Feb 11;17(4):605. doi: 10.3390/cancers17040605. Cancers (Basel). 2025. PMID: 40002200 Free PMC article. Review.
-
The Value of Thin Layer Cytology in Cancer Patients' Pericardial Effusions.Curr Oncol. 2025 May 26;32(6):306. doi: 10.3390/curroncol32060306. Curr Oncol. 2025. PMID: 40558249 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources