

Small fibre pathology, small fibre symptoms and pain in fibromyalgia syndrome
- PMID: 38365860
- PMCID: PMC10873371
- DOI: 10.1038/s41598-024-54365-6
Small fibre pathology, small fibre symptoms and pain in fibromyalgia syndrome
Abstract
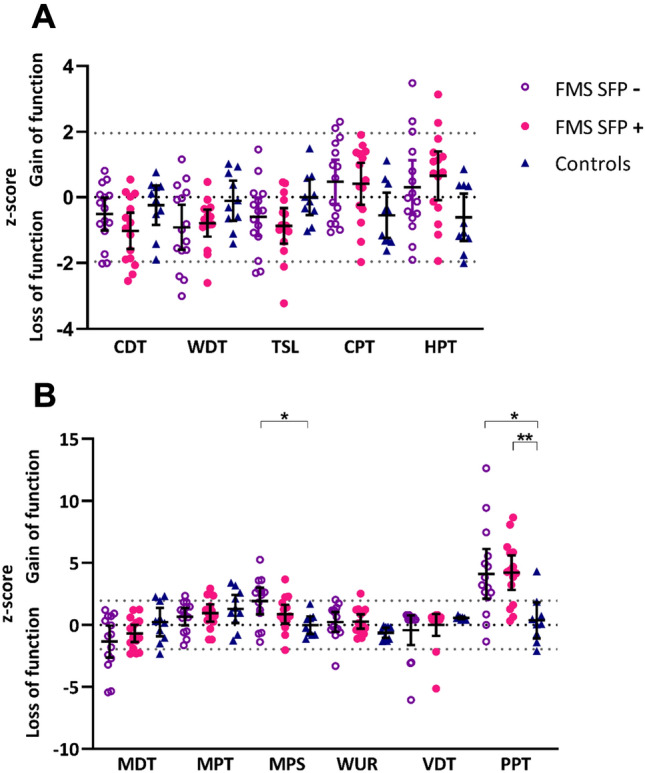
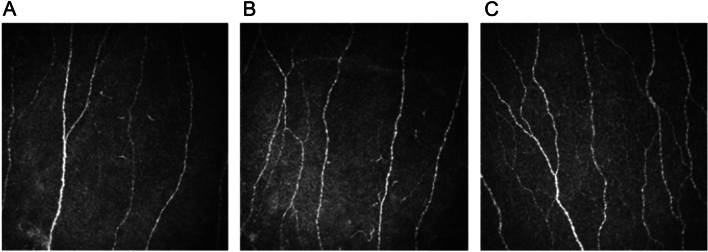
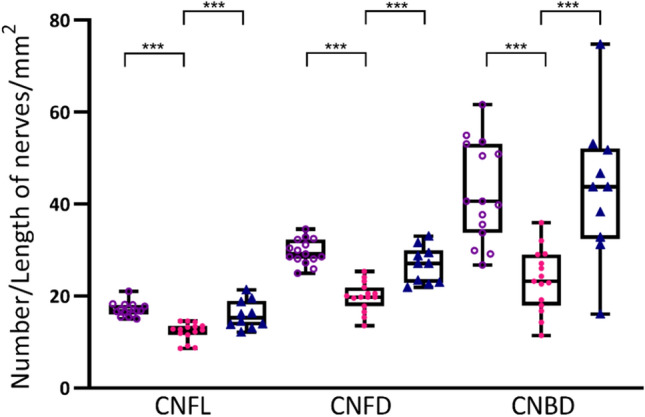
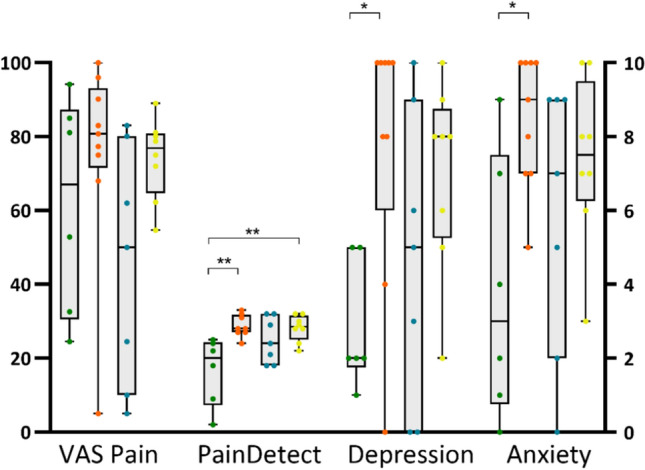
A proportion of people with fibromyalgia demonstrate small fibre pathology (SFP). However, it is unclear how SFP directly relates to pain phenomenology. Thirty-three individuals with FMS and ten healthy volunteers underwent assessment of SFP and sensory phenotyping using corneal confocal microscopy, validated questionnaires and quantitative sensory testing (QST). Corneal nerve fibre length was used to stratify participants with fibromyalgia into with SFP [SFP+] and without SFP [SFP-]. SFP was detected in 50% of the fibromyalgia cohort. Current pain score and QST parameters did not differ between SFP+ and SFP-. Mechanical pain sensitivity (MPS) demonstrated a significant gain-of-function in the SFP- cohort compared to healthy-volunteers (p = 0.014, F = 4.806, η2 = 0.22). Further stratification revealed a cohort without structural SFP but with symptoms compatible with small fibre neuropathy symptoms and a significant gain in function in MPS (p = 0.020 Chi-square). Additionally, this cohort reported higher scores for both depression (p = 0.039, H = 8.483, η2 = 0.312) and anxiety (p = 0.022, F = 3.587, η2 = 0.293). This study confirms that SFP is present in a proportion of people with fibromyalgia. We also show that in a proportion of people with fibromyalgia, small fibre neuropathy symptoms are present in the absence of structural SFP. Greater mechanical pain sensitivity, depression and anxiety are seen in these individuals.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Häuser W, et al. Modified 2016 American College of Rheumatology fibromyalgia criteria, the analgesic, anesthetic, and addiction clinical trial translations innovations opportunities and networks-American Pain Society Pain Taxonomy, and the prevalence of fibromyalgia. Arthritis Care Res. (Hoboken) 2021;73(5):617–625. doi: 10.1002/acr.24202. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
