

Prolyl hydroxylase domain inhibitor is an effective pre-hospital pharmaceutical intervention for trauma and hemorrhagic shock
- PMID: 38365865
- PMCID: PMC10873291
- DOI: 10.1038/s41598-024-53945-w
Prolyl hydroxylase domain inhibitor is an effective pre-hospital pharmaceutical intervention for trauma and hemorrhagic shock
Abstract
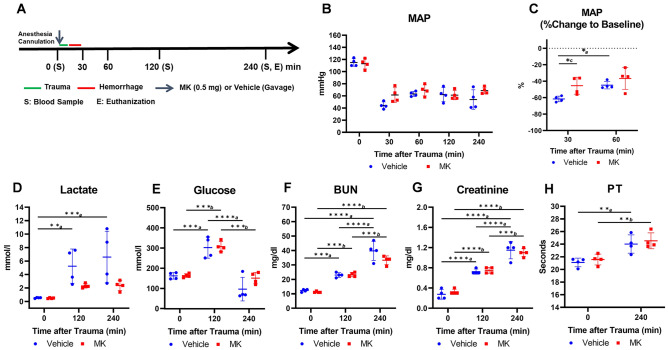
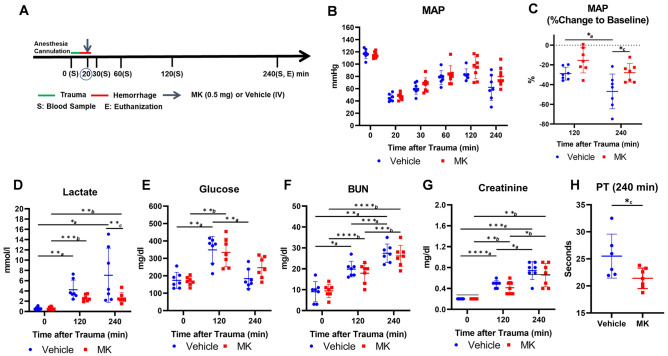
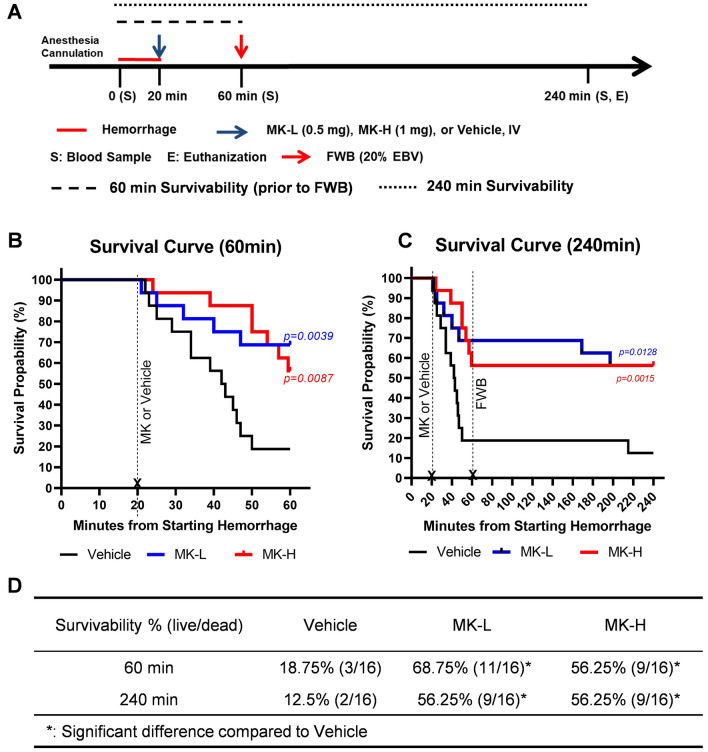
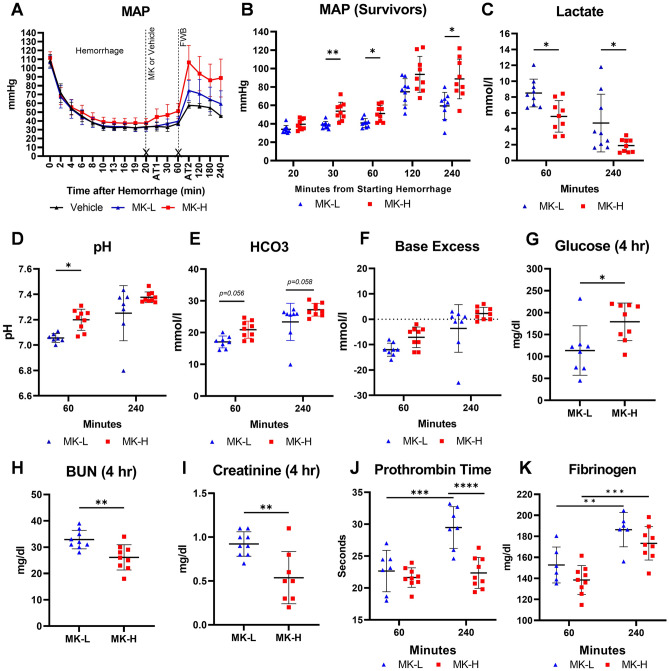
Pre-hospital potentially preventable trauma related deaths are mainly due to hypoperfusion-induced tissue hypoxia leading to irreversible organ dysfunction at or near the point of injury or during transportation prior to receiving definitive therapy. The prolyl hydroxylase domain (PHD) is an oxygen sensor that regulates tissue adaptation to hypoxia by stabilizing hypoxia inducible factor (HIF). The benefit of PHD inhibitors (PHDi) in the treatment of anemia and lactatemia arises from HIF stabilization, which stimulates endogenous production of erythropoietin and activates lactate recycling through gluconeogenesis. The results of this study provide insight into the therapeutic roles of MK-8617, a pan-inhibitor of PHD-1, 2, and 3, in the mitigation of lactatemia in anesthetized rats with polytrauma and hemorrhagic shock. Additionally, in an anesthetized rat model of lethal decompensated hemorrhagic shock, acute administration of MK-8617 significantly improves one-hour survival and maintains survival at least until 4 h following limited resuscitation with whole blood (20% EBV) at one hour after hemorrhage. This study suggests that pharmaceutical interventions to inhibit prolyl hydroxylase activity can be used as a potential pre-hospital countermeasure for trauma and hemorrhage at or near the point of injury.
© 2024. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
A patent was filed: ISR 22-04-US01-PRI: 63/379,518 filed 14 Oct 2022, “Prolyl Hydroxylase Domain Inhibitor Treatment to Improve Survivability of Hemorrhagic Shock” by Andrew P. Cap, James A. Bynum, and Xiaowu Wu from U.S. Army Institute of Surgical Research. The authors declare no competing interests.
Figures

References
-
- Eastridge BJ, Hardin M, Cantrell J, et al. Died of wounds on the battlefield: Causation and implications for improving combat casualty care. J. Trauma. 2011;71:S4–S8. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
