

A first-in-class leucyl-tRNA synthetase inhibitor, ganfeborole, for rifampicin-susceptible tuberculosis: a phase 2a open-label, randomized trial
- PMID: 38365949
- PMCID: PMC10957473
- DOI: 10.1038/s41591-024-02829-7
A first-in-class leucyl-tRNA synthetase inhibitor, ganfeborole, for rifampicin-susceptible tuberculosis: a phase 2a open-label, randomized trial
Abstract
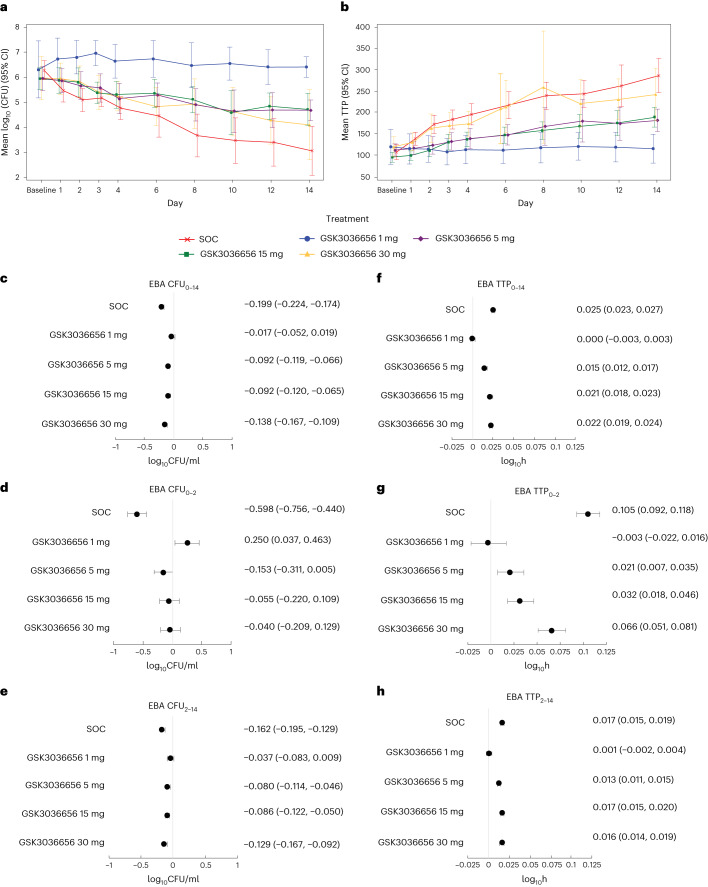
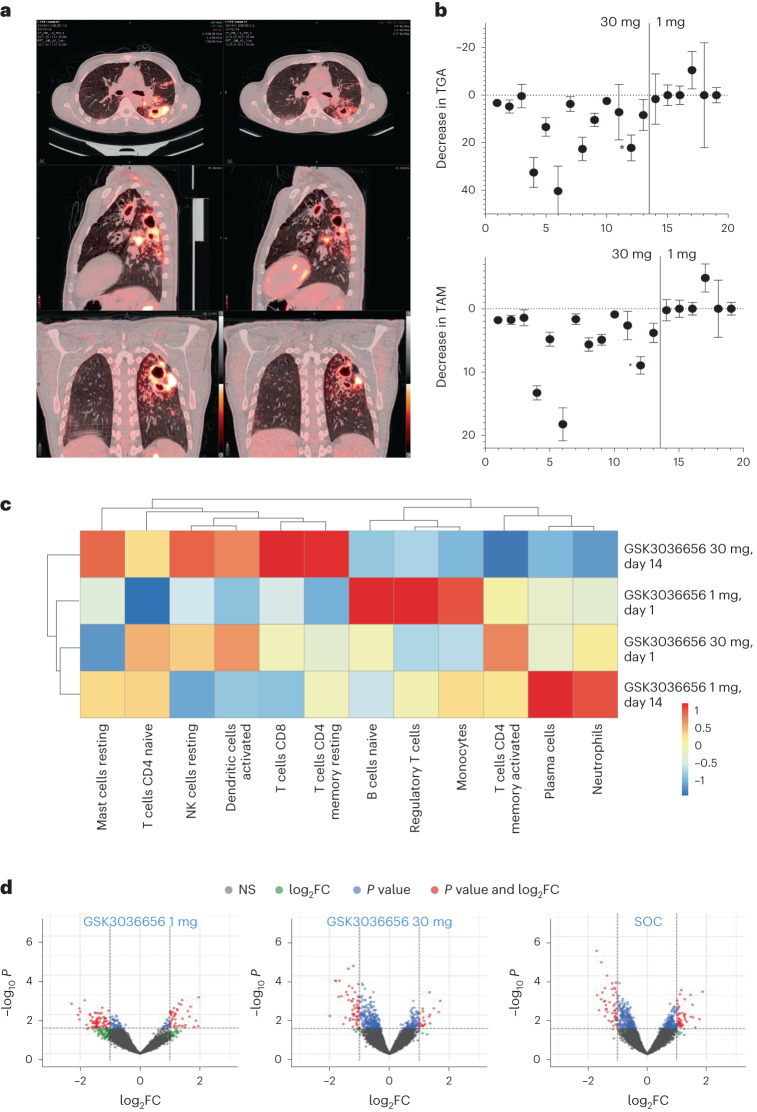
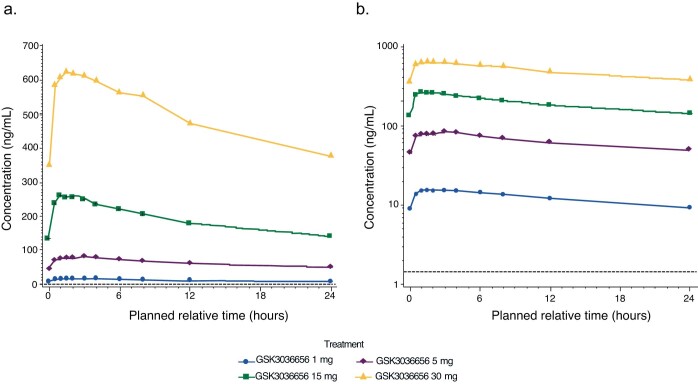
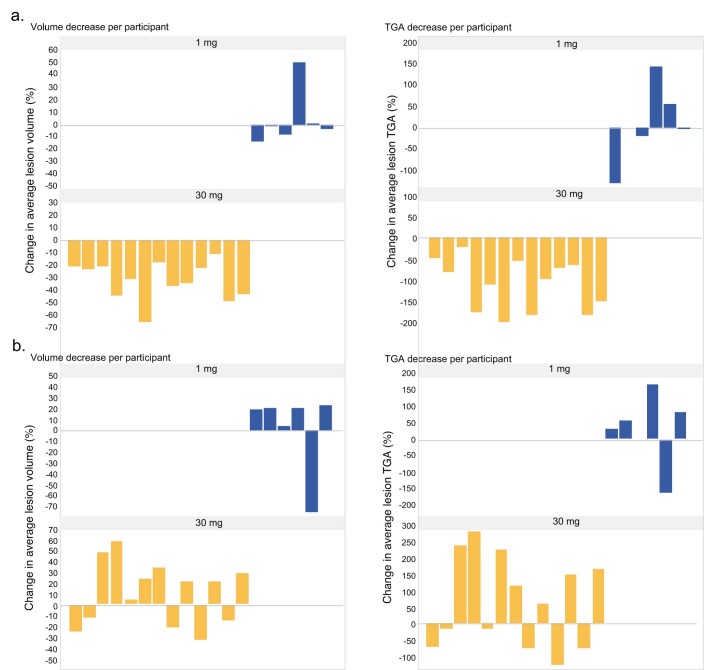
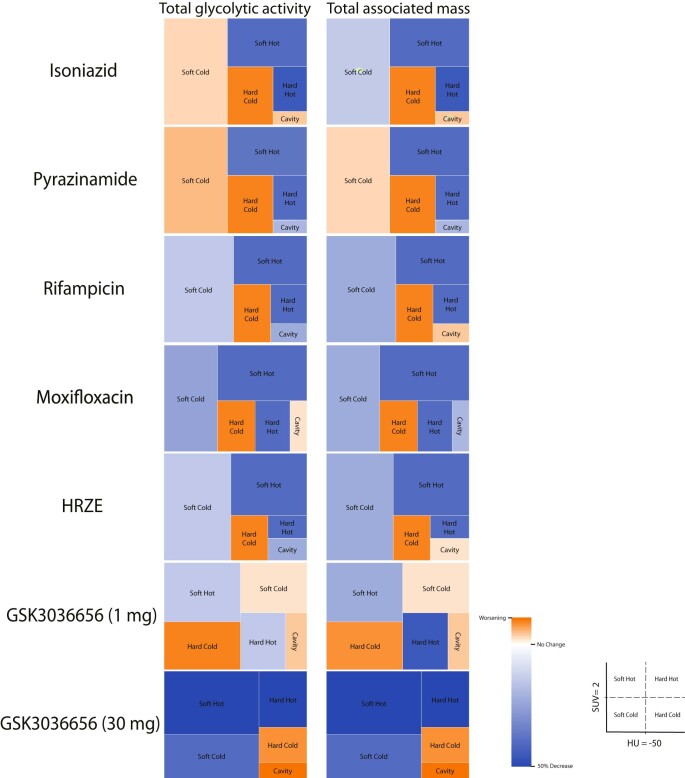
New tuberculosis treatments are needed to address drug resistance, lengthy treatment duration and adverse reactions of available agents. GSK3036656 (ganfeborole) is a first-in-class benzoxaborole inhibiting the Mycobacterium tuberculosis leucyl-tRNA synthetase. Here, in this phase 2a, single-center, open-label, randomized trial, we assessed early bactericidal activity (primary objective) and safety and pharmacokinetics (secondary objectives) of ganfeborole in participants with untreated, rifampicin-susceptible pulmonary tuberculosis. Overall, 75 males were treated with ganfeborole (1/5/15/30 mg) or standard of care (Rifafour e-275 or generic alternative) once daily for 14 days. We observed numerical reductions in daily sputum-derived colony-forming units from baseline in participants receiving 5, 15 and 30 mg once daily but not those receiving 1 mg ganfeborole. Adverse event rates were comparable across groups; all events were grade 1 or 2. In a participant subset, post hoc exploratory computational analysis of 18F-fluorodeoxyglucose positron emission tomography/computed tomography findings showed measurable treatment responses across several lesion types in those receiving ganfeborole 30 mg at day 14. Analysis of whole-blood transcriptional treatment response to ganfeborole 30 mg at day 14 revealed a strong association with neutrophil-dominated transcriptional modules. The demonstrated bactericidal activity and acceptable safety profile suggest that ganfeborole is a potential candidate for combination treatment of pulmonary tuberculosis.ClinicalTrials.gov identifier: NCT03557281 .
© 2024. The Author(s).
Conflict of interest statement
A.C., R.S., G.M.-E., S.T. and M.D. are employees of, and shareholders in, GSK. D.B.A. is an employee of, and shareholder in, GSK, and reports patents planned, issued or pending. S.L.P., G.V. and K.F. are employees of GSK and hold stocks in GSK and Haleon. G.C.K.W.K. is a shareholder in GSK, reports conference fees, expenses and accommodation support from GSK while an employee, and is currently employed by Generate:Biomedicines, Boston, MA, USA. C.L. is supported by the German Center of Infection Research, has provided consultation service to INSMED, has received honoraria for lecturing from INSMED, GILEAD, GSK, MedUpdate and MedUpdateEurope outside of this work, and is a member of the Data Safety Board of trials from Medicines sans Frontiers. C.M.U. received EDCTP grant funding. J.H. received speaker honoraria from GSK and Chiesi, has received support from Boehringer Ingelheim for attending meetings and/or travel, and reports patents planned, issues or pending. A.H.D., I.K., C.E.B., M.R., R.Y.C. and V.d.J. report no conflict of interest.
Figures

References
-
- Tuberculosis Fact Sheet (World Health Organization, 2022).
-
- The END TB Strategy (The World Health Assembly, 2014).
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
