

Neurophysiological signatures of mild traumatic brain injury in the acute and subacute phase
- PMID: 38366159
- PMCID: PMC11176206
- DOI: 10.1007/s10072-024-07364-4
Neurophysiological signatures of mild traumatic brain injury in the acute and subacute phase
Abstract
Background: Mild traumatic brain injury (mTBI) affects 48 million people annually, with up to 30% experiencing long-term complaints such as fatigue, blurred vision, and poor concentration. Assessing neurophysiological features related to visual attention and outcome measures aids in understanding clinical symptoms and prognostication.
Methods: We recorded EEG and eye movements in mTBI patients during a computerized task performed in the acute (< 24 h, TBI-A) and subacute phase (4-6 weeks thereafter). We estimated the posterior dominant rhythm, reaction times (RTs), fixation duration, and event-related potentials (ERPs). Clinical outcome measures were assessed using the Head Injury Symptom Checklist (HISC) and the Extended Glasgow Outcome Scale (GOSE) at 6 months post-injury. Similar analyses were performed in an age-matched control group (measured once). Linear mixed effect modeling was used to examine group differences and temporal changes within the mTBI group.
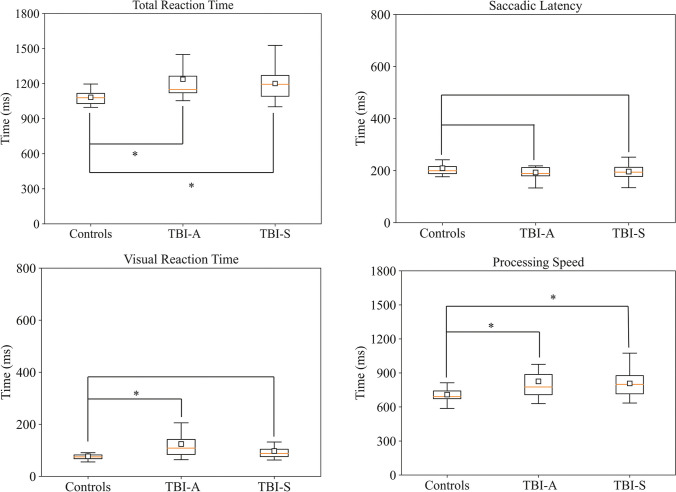
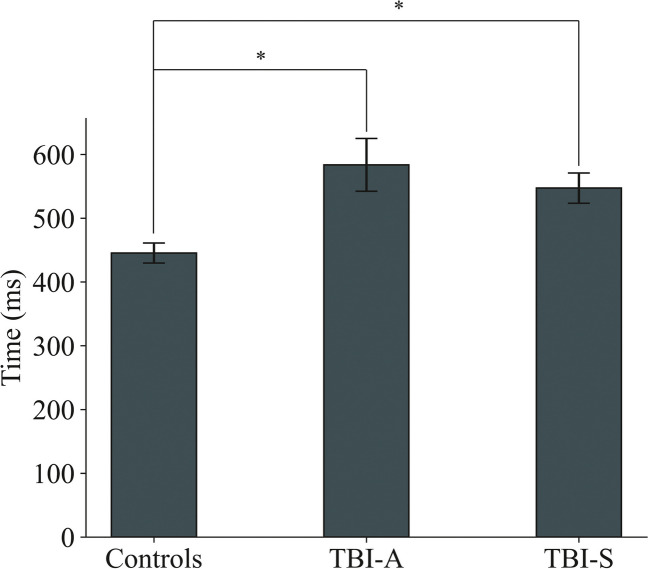
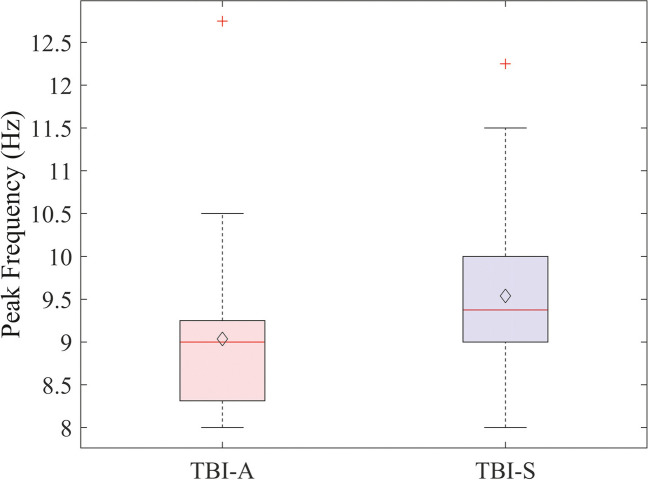
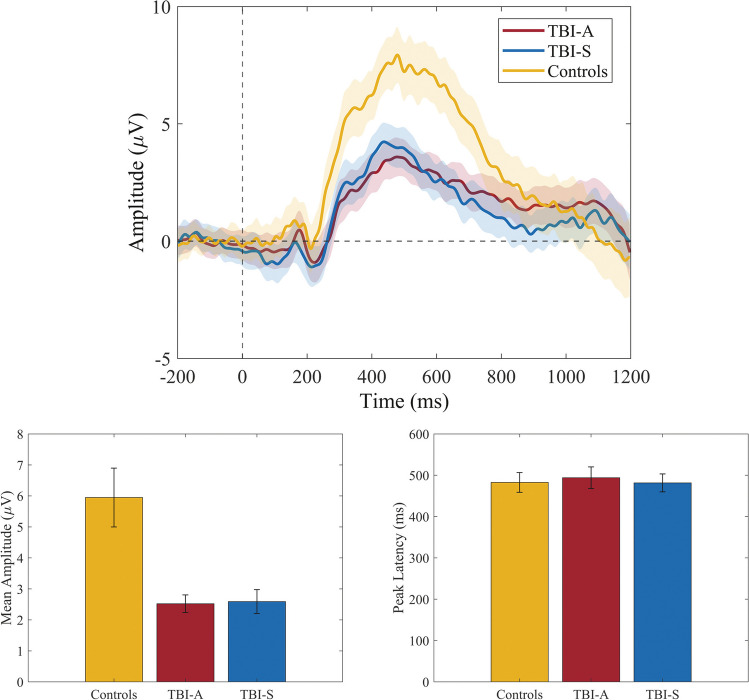
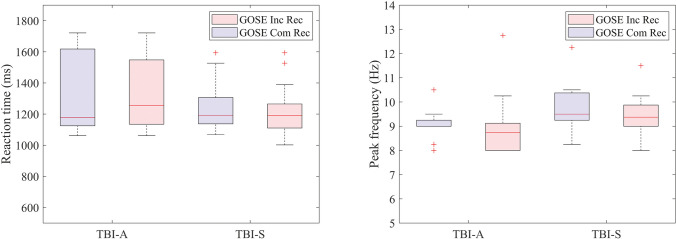
Results: Twenty-nine patients were included in the acute phase, 30 in the subacute phase, and 19 controls. RTs and fixation duration were longer in mTBI patients compared to controls (p < 0.05), but not between TBI-A and TBI-S (p < 0.05). The frequency of the posterior dominant rhythm was significantly slower in TBI-A (0.6 Hz, p < 0.05) than TBI-S. ERP mean amplitude was significantly lower in mTBI patients than in controls. Neurophysiological features did not significantly relate to clinical outcome measures.
Conclusion: mTBI patients demonstrate impaired processing speed and stimulus evaluation compared to controls, persisting up to 6 weeks after injury. Neurophysiological features in mTBI can assist in determining the extent and temporal progression of recovery.
Keywords: EEG; ERP; Eye tracking; Mild traumatic brain injury; Visual attention.
© 2024. The Author(s).
Conflict of interest statement
Michel J.A.M. van Putten is a co-founder of Clinical Science Systems, a manufacturer of clinical EEG software. The remaining authors have no conflicts of interest.
Figures
References
-
- James SA, Ellenbogen RG, Bannick MS, Montjoy-Venning W, Lucchesi LR, Murray CJL. Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990–2016: A systematic analysis for the global burden of disease study 2016. Lancet Neurol. 2019;18:56–87. doi: 10.1016/S1474-4422(18)30415-0. - DOI - PMC - PubMed
-
- Rusnak M (2013) Giving voice to a silent epidemic. Nat Rev Neurol 9(4):186–187 - PubMed
-
- de Koning ME, Gareb B, El Moumni M, Scheenen ME, van der Horn HJ, Timmerman ME, Spikman JM, van der Naalt J. Subacute posttraumatic complaints and psychological distress in trauma patients with or without mild traumatic brain injury. Injury. 2016;47(9):2041–2047. doi: 10.1016/j.injury.2016.04.036. - DOI - PubMed
-
- Hill-Jarrett TG, Gravano JT, Sozda CN, William M (2015) Perl- stein. Visuospatial attention after traumatic brain injury: The role of hemispheric specialization. Brain Injury 29(13–14):1617–1629 - PubMed
-
- Laborey M, Masson F, Ribe´reau-Gayon R, Zongo D, Salmi LR, Lagarde E (2014) Specificity of postconcussion symptoms at 3 months after mild traumatic brain injury: results from a comparative cohort study. J Head Trauma Rehabil 29(1):E28–36 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
