

Deep Learning for Automated Detection and Localization of Traumatic Abdominal Solid Organ Injuries on CT Scans
- PMID: 38366294
- PMCID: PMC11169164
- DOI: 10.1007/s10278-024-01038-5
Deep Learning for Automated Detection and Localization of Traumatic Abdominal Solid Organ Injuries on CT Scans
Abstract
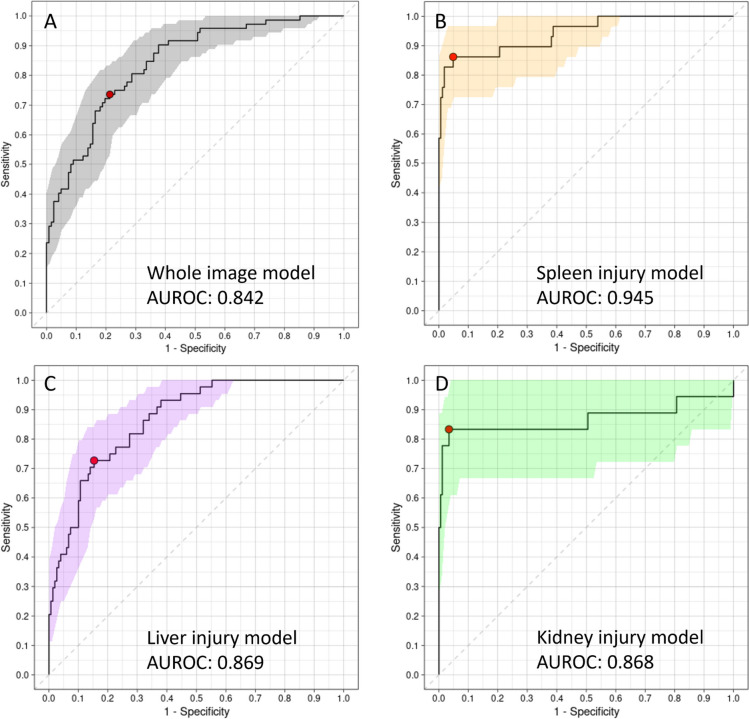
Computed tomography (CT) is the most commonly used diagnostic modality for blunt abdominal trauma (BAT), significantly influencing management approaches. Deep learning models (DLMs) have shown great promise in enhancing various aspects of clinical practice. There is limited literature available on the use of DLMs specifically for trauma image evaluation. In this study, we developed a DLM aimed at detecting solid organ injuries to assist medical professionals in rapidly identifying life-threatening injuries. The study enrolled patients from a single trauma center who received abdominal CT scans between 2008 and 2017. Patients with spleen, liver, or kidney injury were categorized as the solid organ injury group, while others were considered negative cases. Only images acquired from the trauma center were enrolled. A subset of images acquired in the last year was designated as the test set, and the remaining images were utilized to train and validate the detection models. The performance of each model was assessed using metrics such as the area under the receiver operating characteristic curve (AUC), accuracy, sensitivity, specificity, positive predictive value, and negative predictive value based on the best Youden index operating point. The study developed the models using 1302 (87%) scans for training and tested them on 194 (13%) scans. The spleen injury model demonstrated an accuracy of 0.938 and a specificity of 0.952. The accuracy and specificity of the liver injury model were reported as 0.820 and 0.847, respectively. The kidney injury model showed an accuracy of 0.959 and a specificity of 0.989. We developed a DLM that can automate the detection of solid organ injuries by abdominal CT scans with acceptable diagnostic accuracy. It cannot replace the role of clinicians, but we can expect it to be a potential tool to accelerate the process of therapeutic decisions for trauma care.
Keywords: Artificial intelligence; Blunt abdominal trauma; Computed tomography; Deep learning; Liver injury; Renal injury; Spleen injury.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



Similar articles
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Emergency ultrasound-based algorithms for diagnosing blunt abdominal trauma.Cochrane Database Syst Rev. 2015 Sep 14;2015(9):CD004446. doi: 10.1002/14651858.CD004446.pub4. Cochrane Database Syst Rev. 2015. PMID: 26368505 Free PMC article.
-
Development and Validation of a Convolutional Neural Network Model to Predict a Pathologic Fracture in the Proximal Femur Using Abdomen and Pelvis CT Images of Patients With Advanced Cancer.Clin Orthop Relat Res. 2023 Nov 1;481(11):2247-2256. doi: 10.1097/CORR.0000000000002771. Epub 2023 Aug 23. Clin Orthop Relat Res. 2023. PMID: 37615504 Free PMC article.
-
123I-MIBG scintigraphy and 18F-FDG-PET imaging for diagnosing neuroblastoma.Cochrane Database Syst Rev. 2015 Sep 29;2015(9):CD009263. doi: 10.1002/14651858.CD009263.pub2. Cochrane Database Syst Rev. 2015. PMID: 26417712 Free PMC article.
-
Prevalence, characteristics and treatment of concomitant injury to liver and spleen with vascular injury after blunt abdominal trauma.Sci Rep. 2025 Aug 7;15(1):28972. doi: 10.1038/s41598-025-14113-w. Sci Rep. 2025. PMID: 40775260 Free PMC article.
Cited by
-
Artificial Intelligence-What to Expect From Machine Learning and Deep Learning in Hernia Surgery.J Abdom Wall Surg. 2024 Sep 6;3:13059. doi: 10.3389/jaws.2024.13059. eCollection 2024. J Abdom Wall Surg. 2024. PMID: 39310669 Free PMC article. Review.
-
Future Perspectives on Radiomics in Acute Liver Injury and Liver Trauma.J Pers Med. 2024 May 27;14(6):572. doi: 10.3390/jpm14060572. J Pers Med. 2024. PMID: 38929793 Free PMC article. Review.
-
Introduction to Artificial Intelligence for General Surgeons: A Narrative Review.Cureus. 2025 Mar 1;17(3):e79871. doi: 10.7759/cureus.79871. eCollection 2025 Mar. Cureus. 2025. PMID: 40171361 Free PMC article. Review.
-
Artificial intelligence for abdominopelvic trauma imaging: trends, gaps, and future directions.Abdom Radiol (NY). 2025 Mar 21:10.1007/s00261-025-04816-z. doi: 10.1007/s00261-025-04816-z. Online ahead of print. Abdom Radiol (NY). 2025. PMID: 40116889 Free PMC article. Review.
-
Artificial Intelligence in Emergency Trauma Care: A Preliminary Scoping Review.Med Devices (Auckl). 2024 May 23;17:191-211. doi: 10.2147/MDER.S467146. eCollection 2024. Med Devices (Auckl). 2024. PMID: 38803707 Free PMC article.
References
-
- Stassen NA, Bhullar I, Cheng JD, Crandall M, Friese R, Guillamondegui O, et al. Nonoperative management of blunt hepatic injury: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2012;73:S288–S293. doi: 10.1097/TA.0b013e318270160d. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical