

Relevance of lymphocyte proliferation to PHA in severe combined immunodeficiency (SCID) and T cell lymphopenia
- PMID: 38367737
- PMCID: PMC11018339
- DOI: 10.1016/j.clim.2024.109942
Relevance of lymphocyte proliferation to PHA in severe combined immunodeficiency (SCID) and T cell lymphopenia
Abstract
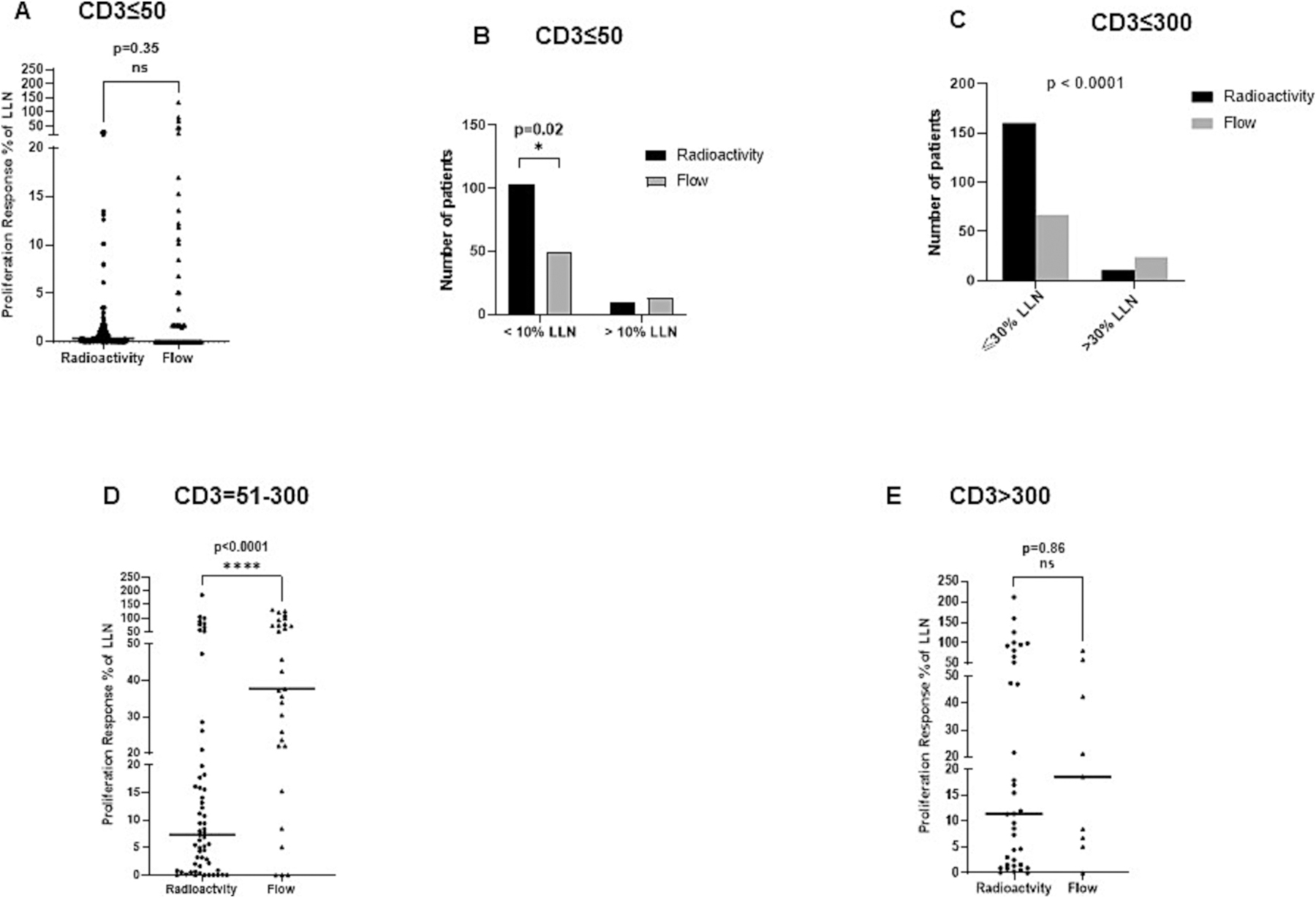
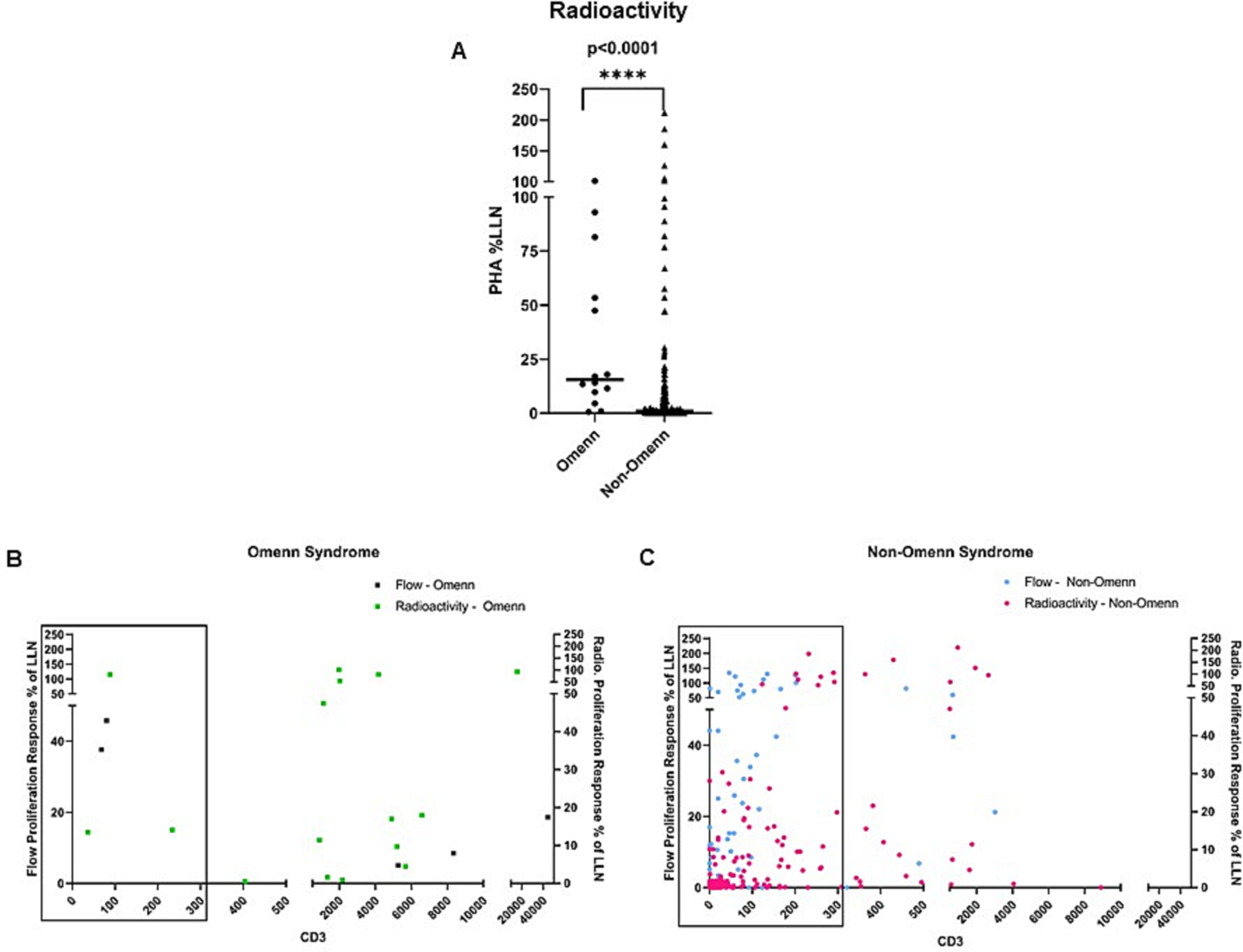
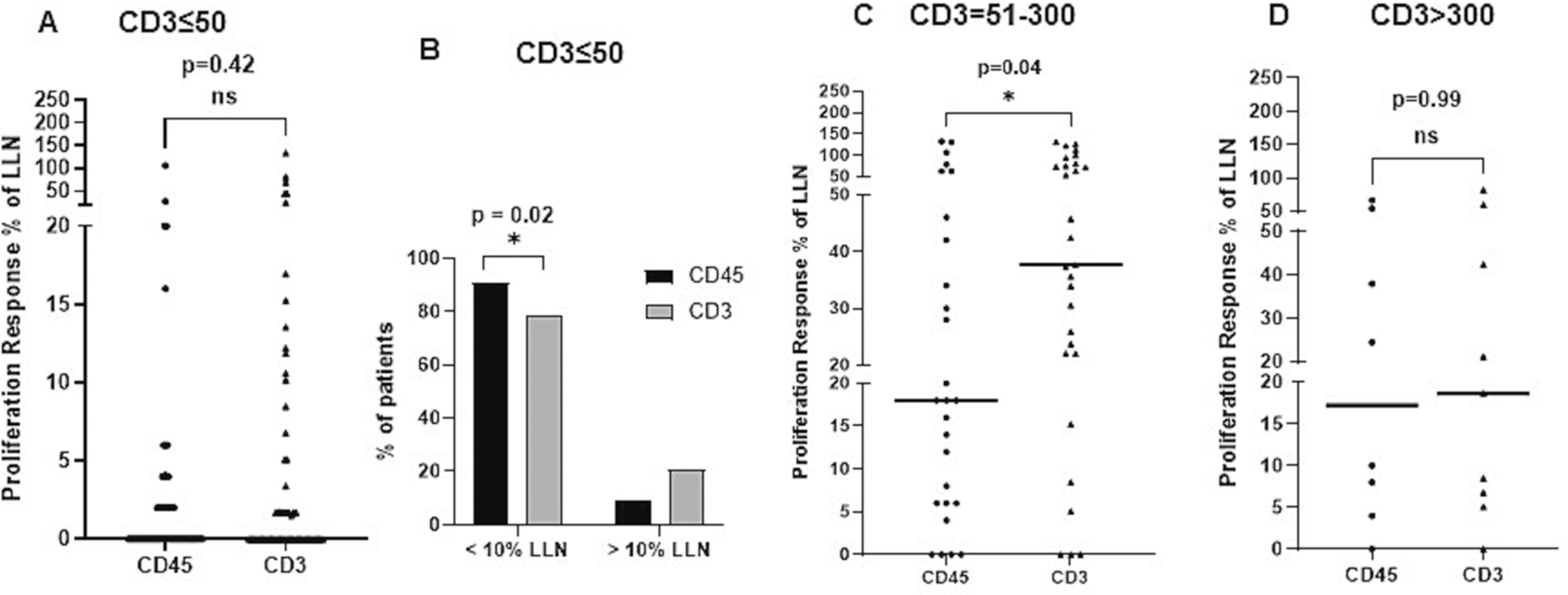
Severe combined immunodeficiency (SCID) is characterized by a severe deficiency in T cell numbers. We analyzed data collected (n = 307) for PHA-based T cell proliferation from the PIDTC SCID protocol 6901, using either a radioactive or flow cytometry method. In comparing the two groups, a smaller number of the patients tested by flow cytometry had <10% of the lower limit of normal proliferation as compared to the radioactive method (p = 0.02). Further, in patients with CD3+ T cell counts between 51 and 300 cells/μL, there was a higher proliferative response with the PHA flow assay compared to the 3H-T assay (p < 0.0001), suggesting that the method of analysis influences the resolution and interpretation of PHA results. Importantly, we observed many SCID patients with profound T cell lymphopenia having normal T cell proliferation when assessed by flow cytometry. We recommend this test be considered only as supportive in the diagnosis of typical SCID.
Keywords: Mitogen; PHA; PIDTC; SCID; Severe combined immunodeficiency; T-cell lymphopenia; T-cell proliferation.
Copyright © 2024 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interest RSA has been on the advisory board for Horizon Pharma (now Amgen) and Sobi in the past 2 years but is not currently serving in that capacity. RM is an employee of Pharming Healthcare Inc., Warren, NJ. JWL is an employee and shareholder of Bluebird Bio, and has been a speaker/consultant and on the advisory board for Sobi, Inc.
Figures



References
-
- Abraham RS, Assessment of functional immune responses in lymphocytes, in: Rich RR, Fleisher TA, Schroeder HW Jr., Weyand CM, Corry DB, Puck JM (Eds.), Clinical Immunology: Principles and Practice, 6th ed., Elsevier, 2022.
-
- Deenick EK, Gett AV, Hodgkin PD, Stochastic model of T cell proliferation: a calculus revealing IL-2 regulation of precursor frequencies, cell cycle time, and survival, J. Immunol 170 (2003) 4963–4972. - PubMed
-
- Bussel JB, Cunningham-Rundles S, LaGamma EF, Shellabarger M, Analysis of lymphocyte proliferative response subpopulations in very low birth weight infants and during the first 8 weeks of life, Pediatr. Res 23 (1988) 457–462. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
