

Diagnosis and treatment of patients with suspected mucinous cystic neoplasms of the liver: a retrospective cohort study
- PMID: 38368313
- PMCID: PMC10874321
- DOI: 10.1007/s00423-024-03246-7
Diagnosis and treatment of patients with suspected mucinous cystic neoplasms of the liver: a retrospective cohort study
Abstract
Purpose: Mucinous cystic neoplasms of the liver (MCN-L) are hepatic cysts with a low malignant potential. The recent European Association for the Study of the Liver (EASL) guidelines provide guidance on the imaging features and surgical management of MCN-L, yet are hampered by a lack of studies adhering to the revised World Health Organization (WHO) criteria. This study attempted to validate the new 2022 EASL-guidelines in a retrospective cohort study of patients who underwent surgery for suspected MCN-L.
Methods: Patients undergoing surgery for suspected MCN-L in a single center between 2010 and 2020 were included. Imaging features were assessed according to the EASL guidelines and were compared to final pathological diagnoses, according to the WHO criteria.
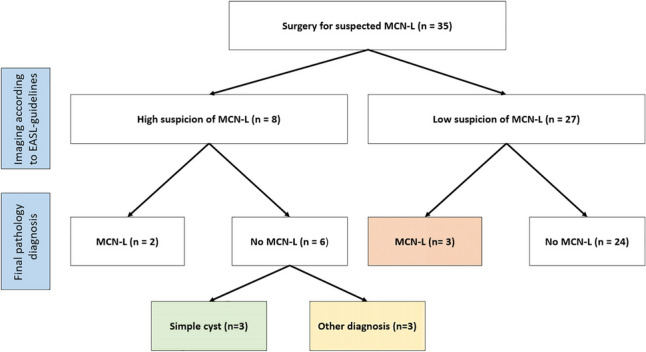
Results: In total, 35 patients were included. In three patients, there were no worrisome imaging features, yet final pathological diagnosis showed MCN-L. Contrarily, six patients with worrisome imaging features did not have MCN-L. Five patients were diagnosed with MCN-L on final pathology. The sensitivity of the EASL-guidelines for the diagnosis of MCN-L was 40% (95%CI: 5.3-85%) and the specificity was 80% (95% CI: 61-92%).
Conclusion: Although the new EASL-guidelines provide some guidance, they could not reliably distinguish MCN-L from other cysts in our series. Thus, preoperative diagnosis of MCN-L remains challenging and we should be careful in selecting surgical strategies based on these criteria.
Keywords: Cyst; Liver; Pathology; Radiology; Surgery.
© 2024. The Author(s).
Conflict of interest statement
None.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
