

Functional outcomes of different surgical treatments for common peroneal nerve injuries: a retrospective comparative study
- PMID: 38368360
- PMCID: PMC10874551
- DOI: 10.1186/s12893-024-02354-x
Functional outcomes of different surgical treatments for common peroneal nerve injuries: a retrospective comparative study
Abstract
Background: This study aims to assess the recovery patterns and factors influencing outcomes in patients with common peroneal nerve (CPN) injury.
Methods: This retrospective study included 45 patients with CPN injuries treated between 2009 and 2019 in Jing'an District Central Hospital. The surgical interventions were categorized into three groups: neurolysis (group A; n = 34 patients), nerve repair (group B; n = 5 patients) and tendon transfer (group C; n = 6 patients). Preoperative and postoperative sensorimotor functions were evaluated using the British Medical Research Council grading system. The outcome of measures included the numeric rating scale, walking ability, numbness and satisfaction. Receiver operating characteristic (ROC) curve analysis was utilized to determine the optimal time interval between injury and surgery for predicting postoperative foot dorsiflexion function, toe dorsiflexion function, and sensory function.
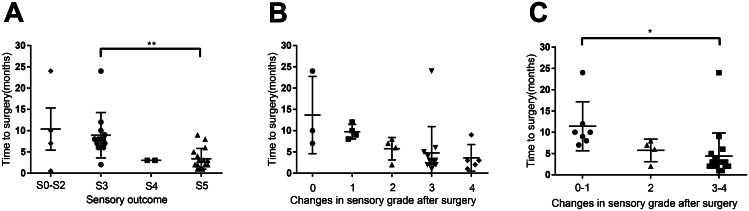
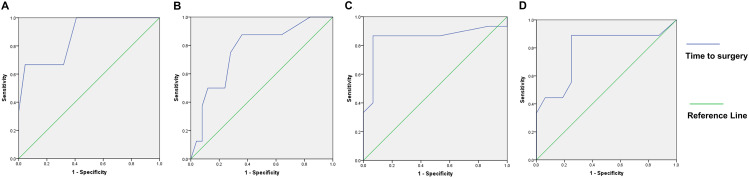
Results: Surgical interventions led to improvements in foot dorsiflexion strength in all patient groups, enabling most to regain independent walking ability. Group A (underwent neurolysis) had significant sensory function restoration (P < 0.001), and three patients in Group B (underwent nerve repair) had sensory improvements. ROC analysis revealed that the optimal time interval for achieving M3 foot dorsiflexion recovery was 9.5 months, with an area under the curve (AUC) of 0.871 (95% CI = 0.661-1.000, P = 0.040). For M4 foot dorsiflexion recovery, the optimal cut-off was 5.5 months, with an AUC of 0.785 (95% CI = 0.575-0.995, P = 0.020). When using M3 toe dorsiflexion recovery or S4 sensory function recovery as the gold standard, the optimal cut-off remained at 5.5 months, with AUCs of 0.768 (95% CI = 0.582-0.953, P = 0.025) and 0.853 (95% CI = 0.693-1.000, P = 0.001), respectively.
Conclusions: Our study highlights the importance of early surgical intervention in CPN injury recovery, with optimal outcomes achieved when surgery is performed within 5.5 to 9.5 months post-injury. These findings provide guidance for clinicians in tailoring treatment plans to the specific characteristics and requirements of CPN injury patients.
Keywords: Common peroneal nerve injury (CPN injury); Nerve repair; Neurolysis; Tendon transfer.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Rasulic L, Savic A, Vitosevic F, Samardzic M, Zivkovic B, Micovic M, Bascarevic V, Puzovic V, Joksimovic B, Novakovic N, et al. Iatrogenic peripheral nerve injuries-Surgical treatment and outcome: 10 years’ experience. World Neurosurg. 2017;103:841–51. doi: 10.1016/j.wneu.2017.04.099. - DOI - PubMed
MeSH terms
Grants and funding
- Nos. 81801941, 82021002, 81830063/National Natural Science Foundation of China
- No. 2021ZD0204200/the National Science and Technology Innovation 2030 Major Program
- No. 21Y11902900/the Shanghai Technology Innovation Plan
- No. 2021Y9129/the Fujian Province Science and Technology Innovation Joint Fund Programme
- No. 2022ZZ01007/the Shanghai Municipal Clinical Medical Center Project
LinkOut - more resources
Full Text Sources
