

Ki-67 labeling index predicts tumor progression patterns and survival in patients with atypical meningiomas following stereotactic radiosurgery
- PMID: 38369575
- PMCID: PMC10978635
- DOI: 10.1007/s11060-023-04537-7
Ki-67 labeling index predicts tumor progression patterns and survival in patients with atypical meningiomas following stereotactic radiosurgery
Abstract
Purpose: This study investigated whether Ki-67 labeling index (LI) correlated with clinical outcomes after SRS for atypical meningiomas.
Methods: This retrospective study examined 39 patients with atypical meningiomas who underwent SRS over a 10-year study period. Ki-67 LI was categorized into 3 groups: low (< 5%), intermediate (5%-10%), and high (> 10%). Local tumor control rates (LCRs), progression-free rates (PFRs), disease-specific survival (DSS) rates, and adverse radiation-induced events (AREs) were evaluated.
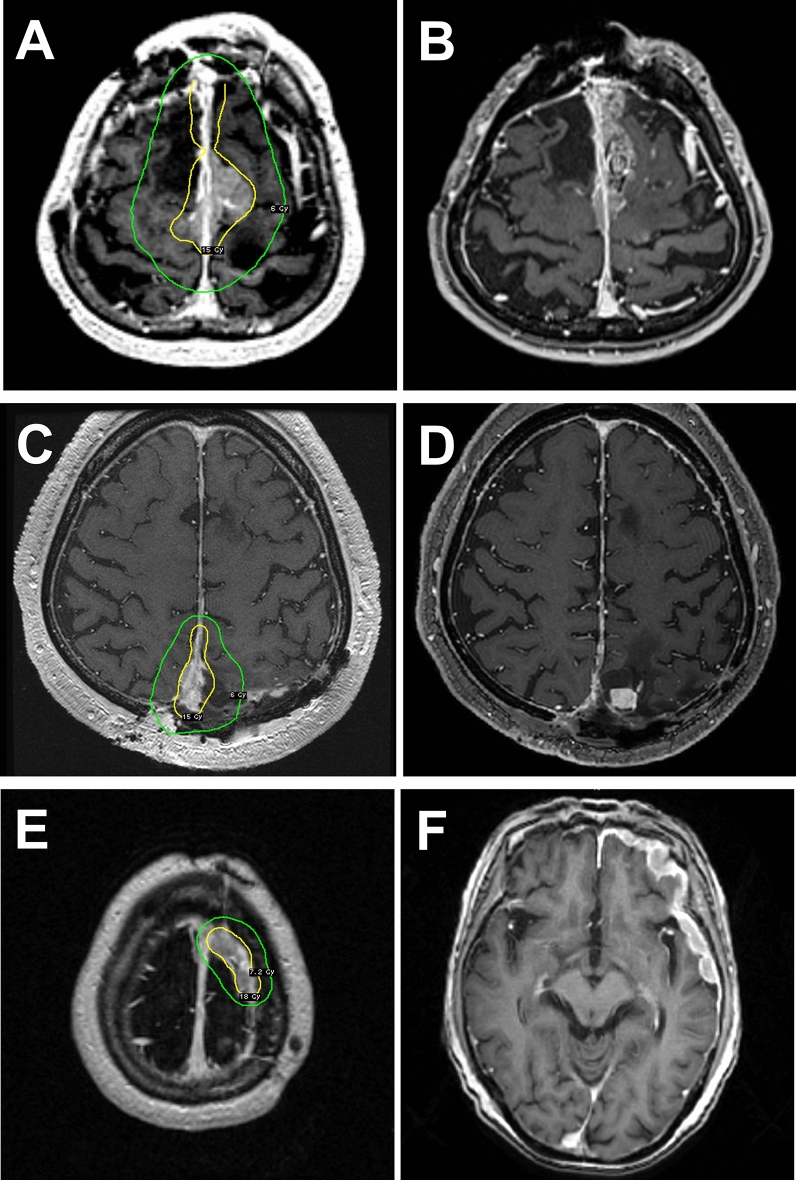
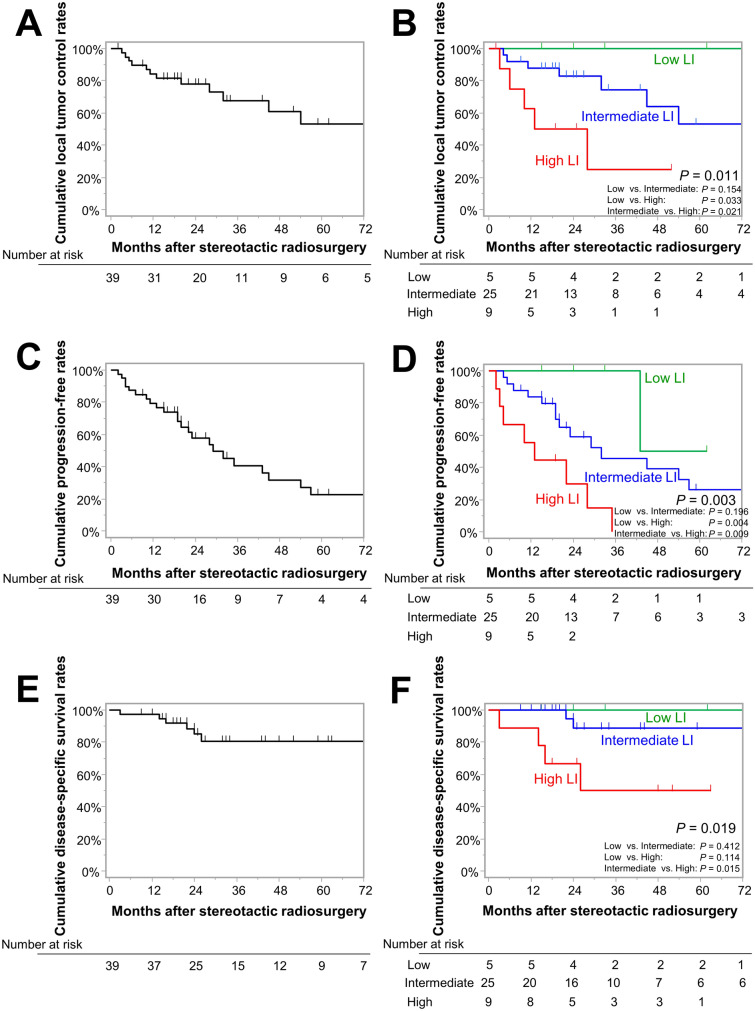
Results: The median follow-up periods were 26 months. SRS was performed at a median prescription dose of 18 Gy for tumors with a median Ki-67 LI of 9.6%. The 3-year LCRs were 100%, 74%, and 25% in the low, intermediate, and high LI groups, respectively (p = 0.011). The 3-year PFRs were 100%, 40%, and 0% in the low, intermediate, and high LI groups (p = 0.003). The 5-year DSS rates were 100%, 89%, and 50% in the low, intermediate, and high LI groups (p = 0.019). Multivariable Cox proportional hazard analysis showed a significant correlation of high LI with lower LCR (hazard ratio [HR], 3.92; 95% confidence interval [CI] 1.18-13.04, p = 0.026), lower PFR (HR 3.80; 95% CI 1.46-9.88, p = 0.006), and shorter DSS (HR 6.55; 95% CI 1.19-35.95, p = 0.031) compared with intermediate LI. The ARE rates were minimal (8%) in the entire group.
Conclusion: Patients with high Ki-67 LI showed significantly more tumor progression and tumor-related death. Ki-67 LI might offer valuable predictive insights for the post-SRS management of atypical meningiomas.
Keywords: Atypical meningioma; Ki-67 labeling index; Recurrence pattern; Stereotactic radiosurgery.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Goldbrunner R, Stavrinou P, Jenkinson MD, Sahm F, Mawrin C, Weber DC, Preusser M, Minniti G, Lund-Johansen M, Lefranc F, Houdart E, Sallabanda K, Le Rhun E, Nieuwenhuizen D, Tabatabai G, Soffietti R, Weller M. EANO guideline on the diagnosis and management of meningiomas. Neuro Oncol. 2021;23:1821–1834. doi: 10.1093/neuonc/noab150. - DOI - PMC - PubMed
-
- Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, Figarella-Branger D, Hawkins C, Ng HK, Pfister SM, Reifenberger G, Soffietti R, von Deimling A, Ellison DW. The 2021 WHO classification of tumors of the central nervous system: a summary. Neuro Oncol. 2021;23:1231–1251. doi: 10.1093/neuonc/noab106. - DOI - PMC - PubMed
-
- Streckert EMS, Hess K, Sporns PB, Adeli A, Brokinkel C, Kriz J, Holling M, Eich HT, Paulus W, Spille DC, van Eck A, Raleigh DR, McDermott MW, Stummer W, Brokinkel B. Clinical, radiological, and histopathological predictors for long-term prognosis after surgery for atypical meningiomas. Acta Neurochir (Wien) 2019;161:1647–1656. doi: 10.1007/s00701-019-03956-8. - DOI - PubMed
