

This is a preprint.
Multiplexed Assays of Variant Effect and Automated Patch-clamping Improve KCNH2-LQTS Variant Classification and Cardiac Event Risk Stratification
- PMID: 38370760
- PMCID: PMC10871451
- DOI: 10.1101/2024.02.01.24301443
Multiplexed Assays of Variant Effect and Automated Patch-clamping Improve KCNH2-LQTS Variant Classification and Cardiac Event Risk Stratification
Update in
-
Multiplexed Assays of Variant Effect and Automated Patch Clamping Improve KCNH2-LQTS Variant Classification and Cardiac Event Risk Stratification.Circulation. 2024 Dec 3;150(23):1869-1881. doi: 10.1161/CIRCULATIONAHA.124.069828. Epub 2024 Sep 24. Circulation. 2024. PMID: 39315434 Free PMC article.
Abstract
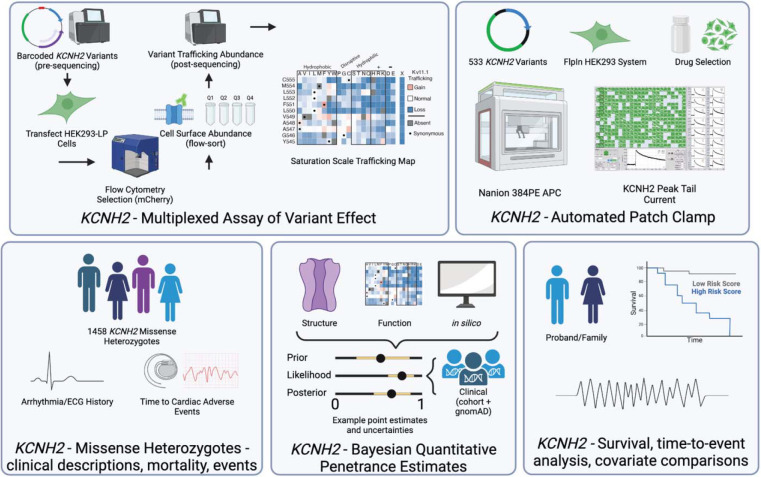
Background: Long QT syndrome (LQTS) is a lethal arrhythmia syndrome, frequently caused by rare loss-of-function variants in the potassium channel encoded by KCNH2. Variant classification is difficult, often owing to lack of functional data. Moreover, variant-based risk stratification is also complicated by heterogenous clinical data and incomplete penetrance. Here, we sought to test whether variant-specific information, primarily from high-throughput functional assays, could improve both classification and cardiac event risk stratification in a large, harmonized cohort of KCNH2 missense variant heterozygotes.
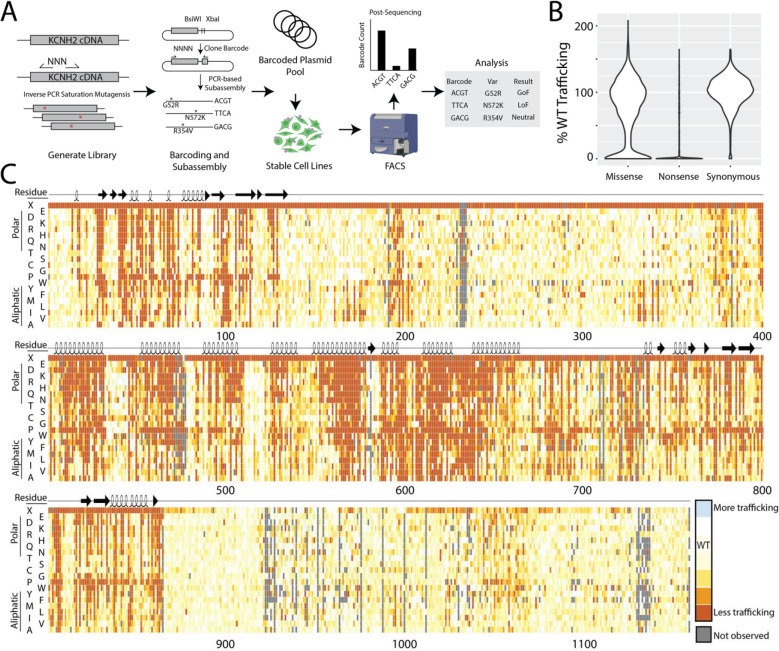
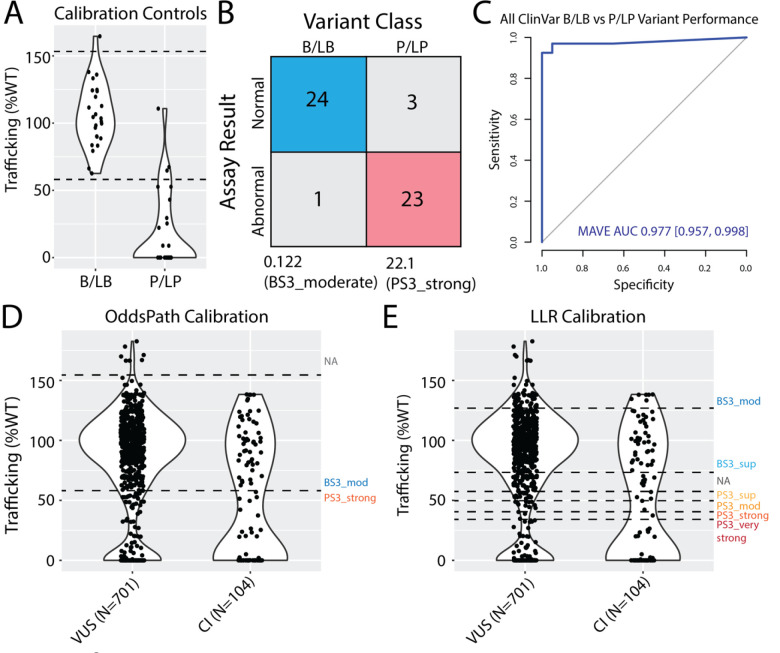
Methods: We quantified cell-surface trafficking of 18,796 variants in KCNH2 using a Multiplexed Assay of Variant Effect (MAVE). We recorded KCNH2 current density for 533 variants by automated patch clamping (APC). We calibrated the strength of evidence of MAVE data according to ClinGen guidelines. We deeply phenotyped 1,458 patients with KCNH2 missense variants, including QTc, cardiac event history, and mortality. We correlated variant functional data and Bayesian LQTS penetrance estimates with cohort phenotypes and assessed hazard ratios for cardiac events.
Results: Variant MAVE trafficking scores and APC peak tail currents were highly correlated (Spearman Rank-order ρ = 0.69). The MAVE data were found to provide up to pathogenic very strong evidence for severe loss-of-function variants. In the cohort, both functional assays and Bayesian LQTS penetrance estimates were significantly predictive of cardiac events when independently modeled with patient sex and adjusted QT interval (QTc); however, MAVE data became non-significant when peak-tail current and penetrance estimates were also available. The area under the ROC for 20-year event outcomes based on patient-specific sex and QTc (AUC 0.80 [0.76-0.83]) was improved with prospectively available penetrance scores conditioned on MAVE (AUC 0.86 [0.83-0.89]) or attainable APC peak tail current data (AUC 0.84 [0.81-0.88]).
Conclusion: High throughput KCNH2 variant MAVE data meaningfully contribute to variant classification at scale while LQTS penetrance estimates and APC peak tail current measurements meaningfully contribute to risk stratification of cardiac events in patients with heterozygous KCNH2 missense variants.
Keywords: LQTS; arrhythmias; automated patch-clamping; multiplexed assay of variant effect; risk stratification.
Figures



References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources