

This is a preprint.
Associations between genetically predicted iron status and cardiovascular disease risk: A Mendelian randomization study
- PMID: 38370765
- PMCID: PMC10871385
- DOI: 10.1101/2024.02.05.24302373
Associations between genetically predicted iron status and cardiovascular disease risk: A Mendelian randomization study
Update in
-
Associations Between Genetically Predicted Iron Status and Cardiovascular Disease Risk: A Mendelian Randomization Study.J Am Heart Assoc. 2024 Jun 4;13(11):e034991. doi: 10.1161/JAHA.124.034991. Epub 2024 May 31. J Am Heart Assoc. 2024. PMID: 38818967 Free PMC article.
Abstract
Background: Mendelian randomization (MR) studies suggest a causal effect of iron (Fe) status on cardiovascular disease (CVD) risk, but it is unknown if these associations are confounded by pleiotropic effects of the instrumental variables (IV) on CVD risk factors. We aimed to investigate the effect of Fe status on CVD risk controlling for CVD risk factors.
Methods: Fe biomarker IVs (total Fe binding capacity (TIBC, n=208,422), transferrin saturation (TSAT, n=198,516), serum Fe (SI, n=236,612), ferritin (n=257,953)) were selected from a European GWAS meta-analysis. We performed two-sample univariate (UV) MR of each Fe trait on CVD outcomes (all-cause ischemic stroke (IS), cardioembolic IS (CES), large artery IS (LAS), small vessel IS (SVS), and coronary heart disease (CHD)) from MEGASTROKE (n=440,328) and CARDIoGRAMplusC4D (n=183,305). We then implemented multivariate (MV) MR conditioning on six CVD risk factors from independent European samples to evaluate their potential confounding and/or mediating effects on the observed Fe-CVD associations.
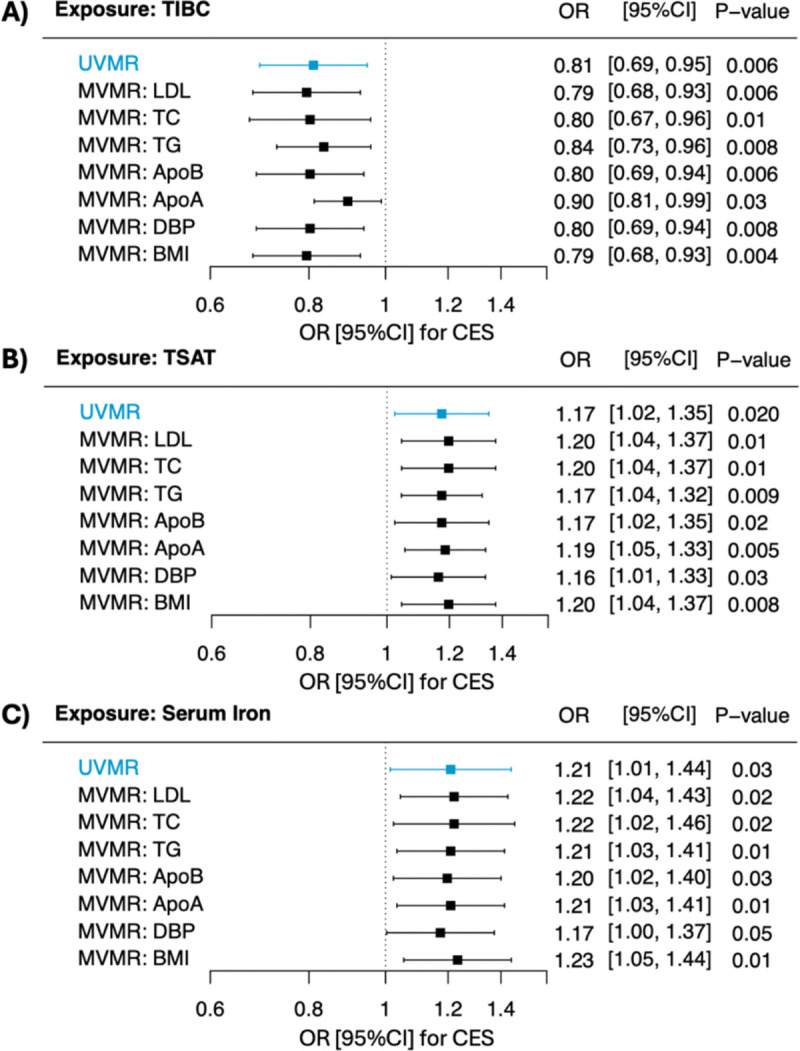
Results: With UVMR analyses, we found higher genetically predicted Fe status to be associated with a greater risk of CES (TSAT: OR 1.17 [95%CI 1.03, 1.33], SI: OR 1.21 [ 95%CI 1.02, 1.44]; TIBC: OR 0.81 [95%CI 0.69, 0.94]). The detrimental effects of Fe status on CES risk remained unaffected when adjusting for CVD risk factors (all P<0.05). Additionally, we found diastolic blood pressure (DBP) to mediate between 7.1-8.8% of the total effect of Fe status on CES incidence. While UVMR initially suggested a protective effect of Fe status on LAS and CHD, MVMR analyses factoring CVD risk factors revealed a complete annulment of this perceived protective effect (all P>0.05).
Discussion: Higher Fe status was associated with a greater risk of CES independent of CVD risk factors, and this effect was partly mediated by DBP. These findings support a role of Fe status as a modifiable risk factor for CES.
Keywords: Mendelian randomization; cardioembolic stroke risk; iron status; ischemic stroke.
Figures


Similar articles
-
Associations Between Genetically Predicted Iron Status and Cardiovascular Disease Risk: A Mendelian Randomization Study.J Am Heart Assoc. 2024 Jun 4;13(11):e034991. doi: 10.1161/JAHA.124.034991. Epub 2024 May 31. J Am Heart Assoc. 2024. PMID: 38818967 Free PMC article.
-
Hypothyroidism's effect on stroke limited to specific subtypes: A Mendelian randomization study.J Stroke Cerebrovasc Dis. 2024 Jul;33(7):107737. doi: 10.1016/j.jstrokecerebrovasdis.2024.107737. Epub 2024 Apr 28. J Stroke Cerebrovasc Dis. 2024. PMID: 38688395
-
Self-Reported Walking Pace and Risk of Cardiovascular Diseases: A Two-Sample Mendelian Randomization Study.Front Genet. 2022 Jun 16;13:871302. doi: 10.3389/fgene.2022.871302. eCollection 2022. Front Genet. 2022. PMID: 35783285 Free PMC article.
-
Mendelian Randomization Study of Heart Failure and Stroke Subtypes.Front Cardiovasc Med. 2022 Apr 7;9:844733. doi: 10.3389/fcvm.2022.844733. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 35463787 Free PMC article.
-
The Application of Mendelian Randomization in Cardiovascular Disease Risk Prediction: Current Status and Future Prospects.Rev Cardiovasc Med. 2024 Jul 11;25(7):262. doi: 10.31083/j.rcm2507262. eCollection 2024 Jul. Rev Cardiovasc Med. 2024. PMID: 39139440 Free PMC article. Review.
References
-
- Masini G, Graham FJ, Pellicori P, Cleland JGF, Cuthbert JJ, Kazmi S, et al. Criteria for Iron Deficiency in Patients With Heart Failure. J Am Coll Cardiol. 2022;79(4):341–51. - PubMed
-
- Fernández-Real JM, Manco M. Effects of iron overload on chronic metabolic diseases. Lancet Diabetes Endocrinol. 2014;2(6):513–26. - PubMed
-
- Oudit GY, Sun H, Trivieri MG, Koch SE, Dawood F, Ackerley C, et al. L-type Ca2+ channels provide a major pathway for iron entry into cardiomyocytes in iron-overload cardiomyopathy. Nat Med. 2003;9(9):1187–94. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources