

This is a preprint.
Localized high-risk prostate cancer harbors an androgen receptor low subpopulation susceptible to HER2 inhibition
- PMID: 38370835
- PMCID: PMC10871443
- DOI: 10.1101/2024.02.09.24302395
Localized high-risk prostate cancer harbors an androgen receptor low subpopulation susceptible to HER2 inhibition
Update in
-
Localized high-risk prostate cancer harbors an androgen receptor activity-low subpopulation susceptible to HER2 inhibition.J Clin Invest. 2025 Sep 4;135(22):e189900. doi: 10.1172/JCI189900. eCollection 2025 Nov 17. J Clin Invest. 2025. PMID: 40906535 Free PMC article. Clinical Trial.
Abstract
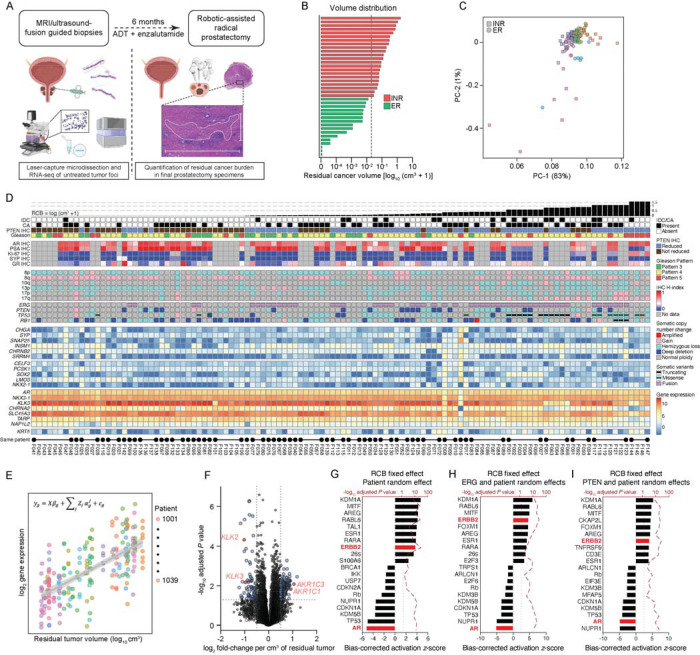
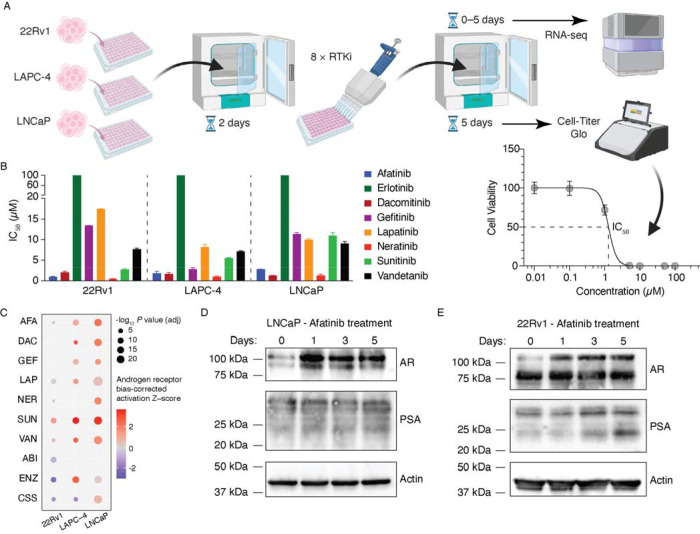
Patients diagnosed with localized high-risk prostate cancer have higher rates of recurrence, and the introduction of neoadjuvant intensive hormonal therapies seeks to treat occult micrometastatic disease by their addition to definitive treatment. Sufficient profiling of baseline disease has remained a challenge in enabling the in-depth assessment of phenotypes associated with exceptional vs. poor pathologic responses after treatment. In this study, we report comprehensive and integrative gene expression profiling of 37 locally advanced prostate tumors prior to six months of androgen deprivation therapy (ADT) plus the androgen receptor (AR) inhibitor enzalutamide prior to radical prostatectomy. A robust transcriptional program associated with HER2 activity was positively associated with poor outcome and opposed AR activity, even after adjusting for common genomic alterations in prostate cancer including PTEN loss and expression of the TMPRSS2:ERG fusion. Patients experiencing exceptional pathologic responses demonstrated lower levels of HER2 and phospho-HER2 by immunohistochemistry of biopsy tissues. The inverse correlation of AR and HER2 activity was found to be a universal feature of all aggressive prostate tumors, validated by transcriptional profiling an external cohort of 121 patients and immunostaining of tumors from 84 additional patients. Importantly, the AR activity-low, HER2 activity-high cells that resist ADT are a pre-existing subset of cells that can be targeted by HER2 inhibition alone or in combination with enzalutamide. In summary, we show that prostate tumors adopt an AR activity-low prior to antiandrogen exposure that can be exploited by treatment with HER2 inhibitors.
Conflict of interest statement
Competing interests H.Y. and R.T.L. perform consulting in an advisory role for Janssen Pharmaceuticals. A.G.S. reports that the National Cancer Institute (NCI) has a Cooperative Research and Development Agreement (CRADA) with Astellas. Resources are provided by this CRADA to the NCI. A.G.S. gets no personal funding from this CRADA but is the primary investigator of the CRADA. The remaining authors declare no conflicts of interest.
Figures



References
-
- Moris L., et al. , Benefits and Risks of Primary Treatments for High-risk Localized and Locally Advanced Prostate Cancer: An International Multidisciplinary Systematic Review. Eur Urol, 2020. 77(5): p. 614–627. - PubMed
-
- Jones C.U., et al. , Radiotherapy and short-term androgen deprivation for localized prostate cancer. N Engl J Med, 2011. 365(2): p. 107–18. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous