

Axillary Lymphadenectomy: Safe Dissection Through a Correct Technique
- PMID: 38371030
- PMCID: PMC10870804
- DOI: 10.7759/cureus.52434
Axillary Lymphadenectomy: Safe Dissection Through a Correct Technique
Abstract
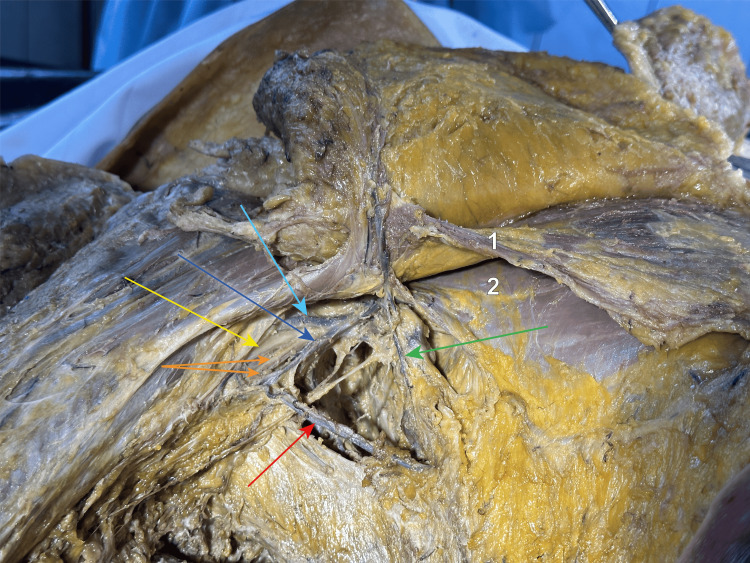
The primary treatment of breast cancer in sentinel-positive ganglia includes axillary lymphatic nodal dissection. The LAD (lymphatic axillary dissection) has decreased in overall numbers but due to the increasing incidence of breast cancer, it is practised on a daily basis, even though there is a myriad of complications such as numbness of the upper limb and chest wall, movement restriction of the upper limb, and chronic pain which appear due to trauma to the nerves which pass through the axilla. However, the utility in the overall survival or DFS (disease-free survival) of the patient is unquestionable. In our study, through the dissection of cadavers, we exposed the vital structures and the anatomical relations of this region. We aimed to offer a map or technique for the surgeon to follow to decrease the overall morbidity of this procedure.
Keywords: breast and endocrine surgery; breast conservation therapy; breast disease; en bloc breast implant removal; thoracic and breast oncology - areas of interest.
Copyright © 2024, Slavu et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




References
-
- Sentinel lymph node methods in breast cancer. Giammarile F, Vidal-Sicart S, Paez D, et al. Semin Nucl Med. 2022;52:551–560. - PubMed
-
- Controversies in axillary treatment of breast cancer patients and metastatic sentinel lymph node. Novoa AG, Nebril BA. J Cancer Sci Ther. 2016;8:66–68.
-
- The decline of axillary lymph node dissection in breast cancer. Evolution of its indication over the last 20 years. García-Novoa A, Acea-Nebril B, Casal-Beloy I, et al. Cir Esp (Engl Ed) 2019;97:222–229. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials