

Relapse of COVID-19 and Viral Evolution in a Patient With Good Syndrome: A Case Report
- PMID: 38371040
- PMCID: PMC10874686
- DOI: 10.7759/cureus.52592
Relapse of COVID-19 and Viral Evolution in a Patient With Good Syndrome: A Case Report
Abstract
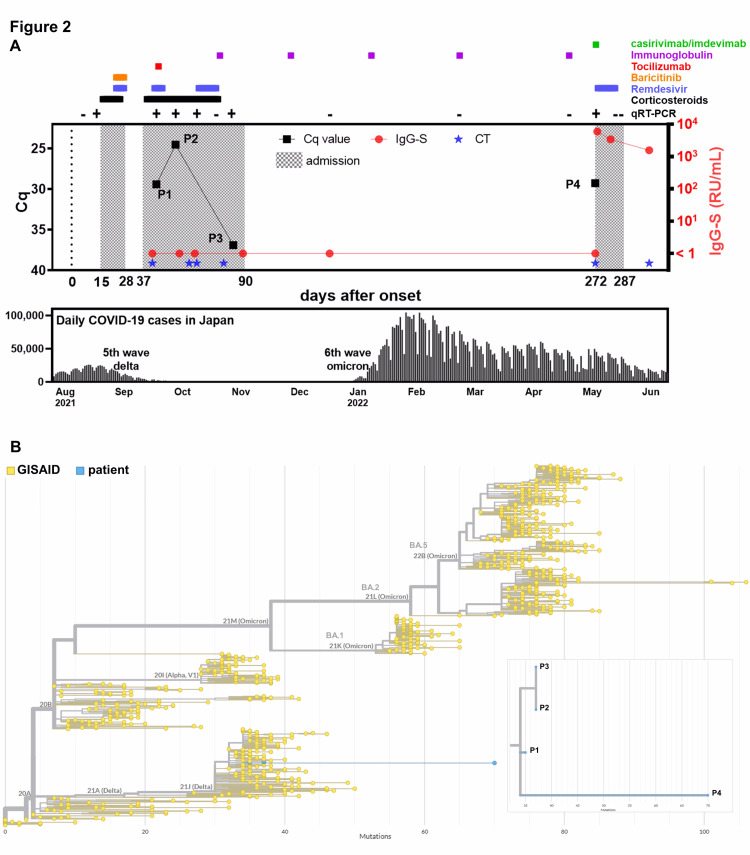
Delays in clearance and rapid evolution of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have been reported in immunocompromised patients. We encountered a case of recurrent, multi-mutational SARS-CoV-2 infection in a 40-year-old man with severe immunodeficiency due to Good syndrome. The patient had not received the SARS-CoV-2 vaccination. In August 2021, he was first admitted to the hospital owing to coronavirus disease 2019 (COVID-19) pneumonia and was administered dexamethasone, remdesivir, and baricitinib. Although his fever and respiratory condition improved once, chest computed tomography (CT) revealed extensive diffuse consolidation and ground-glass opacities (GGOs), and both methylprednisolone pulse therapy and tocilizumab yielded a limited effect. After a third course of remdesivir without immunosuppressants or steroids, the patient recovered, and he tested negative for SARS-CoV-2. On day 272 since the clinical onset, he was readmitted with dyspnea and mild fever due to a COVID-19 recurrence. He was infected with the Delta variant (AY.29), despite the Omicron (BA.2) variant being predominant at that time. During this admission, additional remdesivir and casirivimab/imdevimab yielded marked effects, and the SARS-CoV-2 quantitative reverse transcriptase-polymerase chain reaction (qRT-PCR) tests rapidly returned negative. Phylogenetic analysis demonstrated the accumulation of mutations, including those yielding remdesivir resistance, throughout the SARS-CoV-2 genome. Appropriate use of antivirals and monoclonal antibodies may aid in the recovery of patients with COVID-19 and immunodeficiency and in preventing the emergence of multi-mutational SARS-CoV-2 variants.
Keywords: covid-19; good syndrome; relapse; sars-cov-2; viral evolution.
Copyright © 2024, Iwasaki et al.
Conflict of interest statement
The authors have declared financial relationships, which are detailed in the next section.
Figures


References
-
- Underlying medical conditions associated with higher risk for severe COVID-19: information for healthcare professionals. [ May; 2023 ]. 2023. https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/underlyingco... https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/underlyingco...
-
- Outbreak.info. (2023) [ May; 2023 ]. 2023. https://outbreak.info https://outbreak.info
-
- Good syndrome: an adult-onset immunodeficiency remarkable for its high incidence of invasive infections and autoimmune complications. Malphettes M, Gérard L, Galicier L, et al. Clin Infect Dis. 2015;61:0–9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous